

A 28-year-old man with multiple gunshot wounds to the chest and upper extremities was transported by private vehicle to a community hospital with limited trauma capabilities. On arrival he developed pulseless electrical activity and cardiopulmonary resuscitation was initiated. He was intubated, transfused with 4 units of packed red blood cells, and resuscitated with 2 L of crystalloid prior to regaining spontaneous circulation. Left-sided tube thoracostomy immediately drained 1600 mL of bright red blood. He was transiently stable for a short transport to the nearest level 1 trauma center.
On arrival the patient was normotensive with tachycardia. Chest X-ray demonstrated persistent left-sided hemothorax despite a well-positioned chest tube. Focused Assessment with Sonography for Trauma (FAST) examination was negative for pericardial fluid, but positive for intra-abdominal fluid. During the secondary examination the patient became hypotensive with systolic blood pressure (SBP) in the 70 s. A massive transfusion protocol was initiated, tranexamic acid was administered, and the patient was promptly transported to the operating room.
The patient transiently responded to the massive transfusion. While instruments were being opened in the operating room, he again became hypotensive with SBP in the 50 s. The patient was acidotic (pH of 6.87, base excess −14.6), coagulopathic (international normalized ratio of 1.5) and hypothermic (core body temperature, 32.8°C).
What would you do as an immediate next step?
Exploratory laparotomy.
Aggressive fluid and blood product resuscitation to improve BP prior to induction of anesthesia.
Resuscitative thoracotomy with aortic cross-clamping.
Retrograde endovascular balloon occlusion of the aorta (REBOA).
What We Did and Why
Correct answer: D
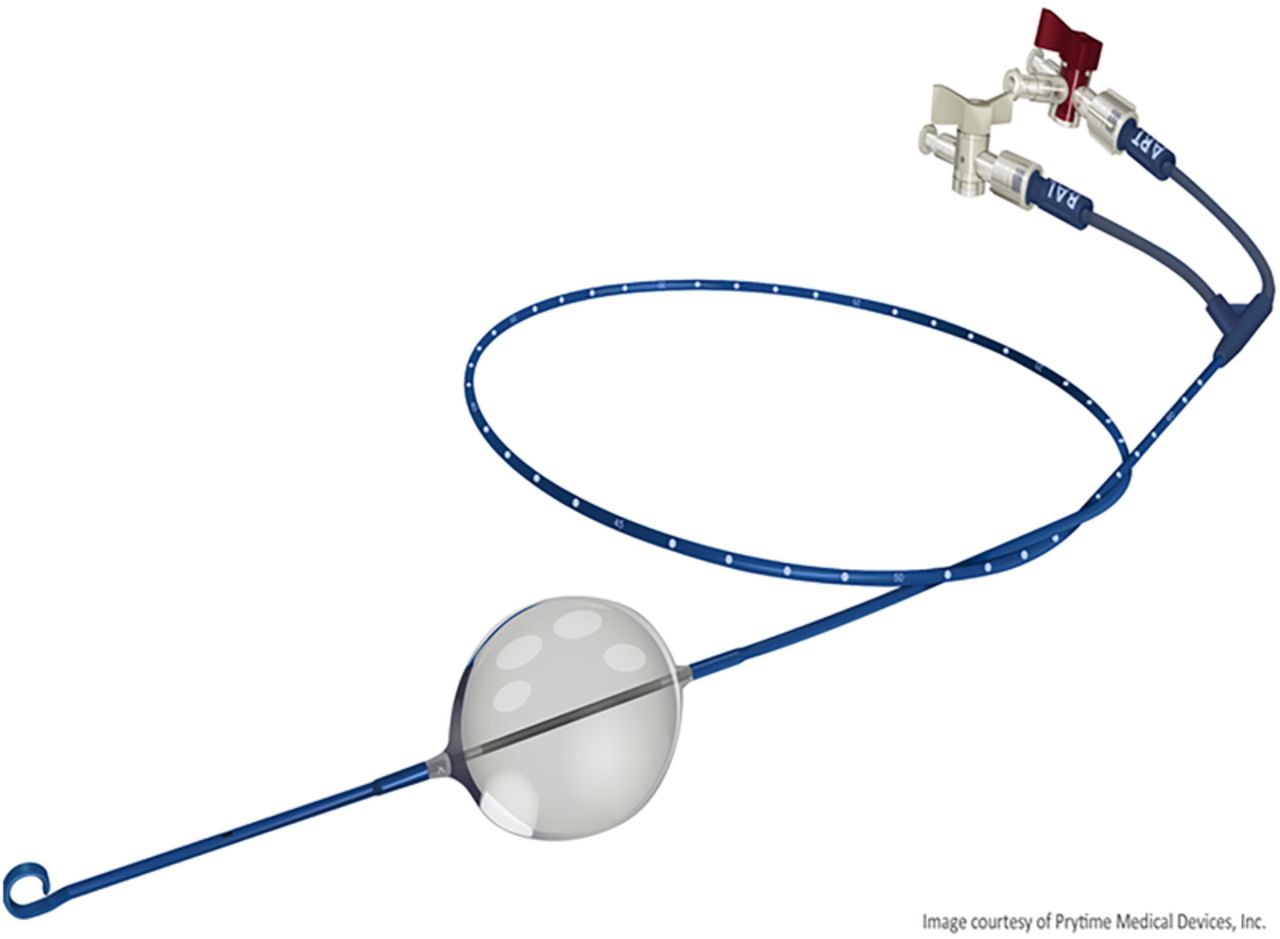
Rather than perform a thoracotomy with open aortic cross-clamping or an exploratory laparotomy, we inserted a readily available low profile REBOA catheter (ER-REBOA, Prytime Medical, Boerne, Texas, USA; figure 1) into the right common femoral artery via cut down to expedite access. The catheter was advanced into the descending thoracic aorta (zone I) and completely inflated for 8 min. The time from incision to balloon inflation was 3 min and 10 s. There was an immediate rise in SBP to 140 mm Hg on complete aortic occlusion. With transfusion of blood products ongoing, simultaneous left anterolateral thoracotomy and exploratory laparotomy were initiated. A large hemothorax was evacuated from the left chest. A transpulmonary gunshot wound tract was identified, with associated severe injury to the lower lobe of the lung. Non-anatomic resection was performed. After control of hemorrhage, the REBOA balloon's position was confirmed within the descending thoracic aorta by palpation. Laparotomy revealed moderate hemoperitoneum due to a significant splenic injury that required splenectomy.

ER-REBOA catheter. Design features include low-profile 7 French sheath designed for percutaneous insertion, stiff catheter that does not require the Seldinger technique or a guide-wire for insertion, curled catheter tip to minimize aortic injury and malposition, centimeter markings on the catheter to aid in blind positioning, and a proximal aortic blood pressure transducer.
Following control of major sources of hemorrhage, balloon inflation volume was gradually reduced to provide slow transition from full to partial aortic occlusion while the operation was ongoing. The balloon was initially manually deflated with a syringe until partial distal blood flow was confirmed by the return of a palpable distal pulse in the abdominal aorta. Thereafter, the balloon was sequentially deflated in 1 mL intervals per minute as hemodynamically tolerated. In total, partial occlusion continued for 20 min until definitive hemorrhage control was achieved (figure 2). No vasopressors were used in the operating room. After arrival to the intensive care unit (ICU) the patient was alert and able to follow commands. Early hemodynamics and laboratory data are listed in table 1. The patient was transferred out of the ICU on hospital day 5 and discharged on hospital day 13.

Graph of intraoperative variation in mean arterial pressure (MAP) as measured in the radial arterial. Important corresponding events during the course of REBOA therapy are indicated. REBOA, Retrograde Balloon Occlusion of the Aorta.
Selected vital signs and laboratory results from arrival to the operating room through early resuscitation in the intensive care unit
REBOA is an emerging, less invasive alternative to resuscitative thoracotomy with aortic cross-clamping for the treatment of severe truncal hemorrhage. While its use is increasing, REBOA is associated with similar deleterious effects from complete aortic occlusion, including proximal hypertension, distal ischemia, and systemic ischemia-reperfusion injury. New approaches to endoluminal aortic occlusion are evolving to address these consequences. The emerging technique of partial REBOA (P-REBOA), utilized in this patient, minimizes truncal hemorrhage, preserves distal perfusion, and avoids hemodynamic extremes caused by complete aortic occlusion. Allowing blood flow beyond the balloon may alleviate supraphysiological proximal pressures while maintaining a degree of distal organ perfusion, mitigating the systemic burden of ischemia-reperfusion as observed in this patient (table 1).
This case represents the first reported survival of a trauma patient resuscitated with a new low profile REBOA catheter able to be placed through a 7 French arterial sheath, and is the first clinical report of the use of P-REBOA in the USA. The new low profile ER-REBOA catheter and the technique of P-REBOA appear to have some benefit over current balloon catheters and the technique of complete REBOA. Ongoing efforts should continue to optimize this approach and develop clear algorithms for its use.
Footnotes
Contributors AJD, RMR, JJD, GJJ and JMG conducted literature search. JJD and JR handled the clinical case. AJD, RMR, JJD, GJJ and JMG were involved in writing the manuscript. AJD, RMR, JJD, JR, GJJ and JMG carried out the critical revision of the manuscript.
Disclaimer The views expressed in this material are those of the authors, and do not reflect the official policy or position of the U.S. Government, the Department of Defense, the Department of the Air Force, or the University of California Davis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/




{kind=link}
{kind=link}