

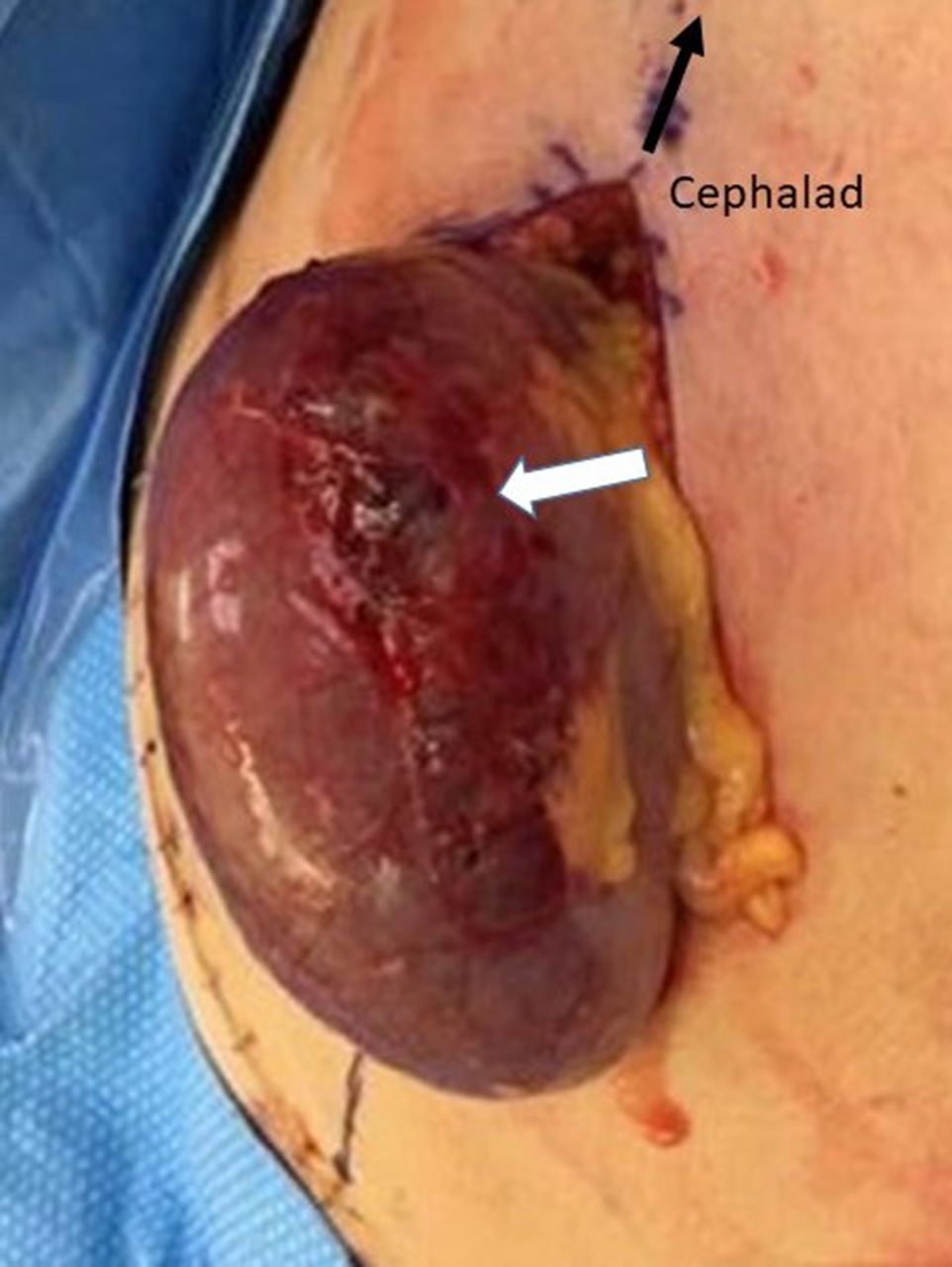
A 55-year-old woman with end-stage renal disease secondary to IgA nephropathy underwent an uneventful de novo deceased-donor kidney transplantation under induction with intravenous solumedrol 250 mg × 2 and antithymocyte globulin 1.5 mg × 2. Postoperative renal allograft sonography was unremarkable and she continued to make adequate urine. An immunosuppressive regimen with tacrolimus maintained at a level of 8–10 ug/L, mycophenolate mophetil 1000 mg two times per day, and prednisone 10 mg po once daily was started. On the third postoperative day, the patient developed abdominal distention and inability to tolerate oral intake. Initial abdominal CT scan showed prominent colonic distention involving portions of the small bowel but no mechanical obstruction. With conservative management, the abdominal distention and pain continued to progress with increasing sinus tachycardia. A repeat CT scan demonstrated a cecal diameter of 12 cm, with small foci of extra luminal air along the ascending colon, and a small amount of free fluid throughout the peritoneal cavity but no contrast extravasation. Decision was made to proceed with a diagnostic laparoscopy. Intraoperatively, it was converted to an open laparotomy because of unexpected finding of cecal volvulus (figure 1) with ischemia (figure 2).
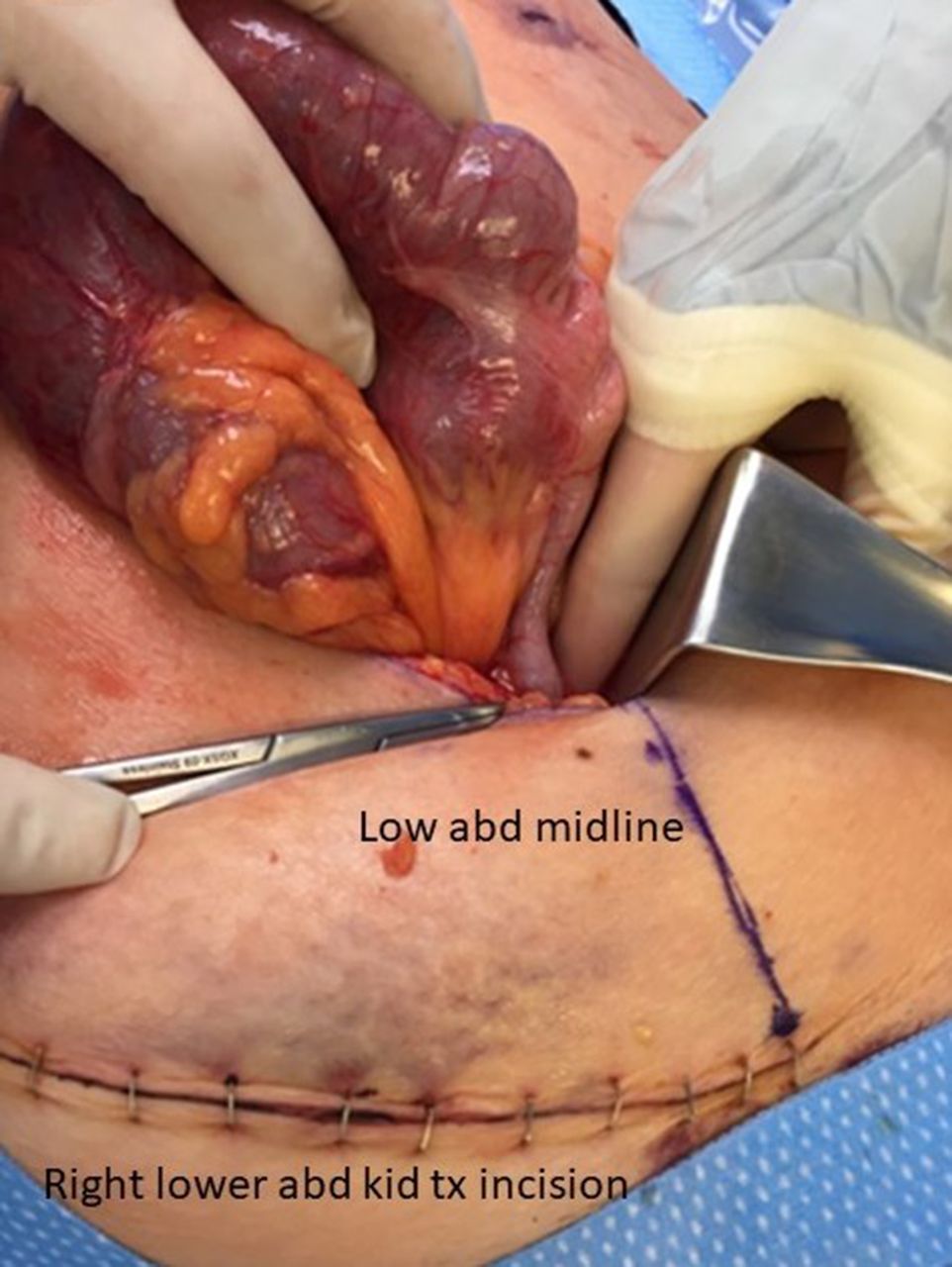
Intraoperative finding of cecal volvulus. Noted that the cecum rotated counterclockwise. The base of the appendix was pointing to the left lower quadrant of the abdomen. abd, abdomen; kid, kidney.

Ischemic change of the cecum secondary to volvulus, with focal necrosis and impending perforation on the anterior cecal wall (white arrow).
What would you do?
Right hemicolectomy, diverting end ileostomy.
Right hemicolectomy, ileocolostomy with proximal diverting loop ileostomy.
Right hemicolectomy, ileocolostomy without proximal ileostomy.
What we did and why
Correct answer C
We performed a right hemicolectomy with primary stapled ileocolostomy with no diversion. Postoperatively, the prednisone dose was reduced to 5 mg po once daily, and the mycophenolate mophetil dose was reduced to 750 mg twice daily. Even though the postoperative course was protracted with a prolonged ileus as well as persistent tachycardia and leukocytosis, she did not develop an anastomotic leak and was discharged home with a functional kidney allograft on postoperative day 15.
Management of cecal volvulus with ischemia in the renal transplant recipient is challenging. The need for a proximal flow diversion after segmental colectomy remains controversial.
The effects of immunosuppression on wound and bowel anastomosis healing have been studied vastly but the measurement of a clinical effect has been challenging due to the use of multidrug regimens. Not all immunosuppressive drugs have demonstrated a negative impact on colonic anastomosis healing. Interestingly, tacrolimus, a calcineurin inhibitor, has not demonstrated a negative impact on colonic anastomotic healing in vivo studies, whereas sirolimus and everolimus have been implicated in poor wound and intestinal anastomotic healing. Studies on mycophenolate mofetil have reported conflicting results in its impact, but a recent in vivo study has demonstrated no negative effect on intestinal anastomosis but a possible negative effect on abdominal wall healing. As far as steroid is concerned, several studies have documented increased leak rates in left-sided colonic anastomoses in patients receiving chronic glucocorticoid therapy. Although the use of high doses of perioperative corticosteroids in transplant patients has been linked to an increased risk ofcomplication in colonic anastomosis as compared with the general population, the rates of complication are lower than those on chronic steroid therapy.
On the other hand, anastomosis diversion in the form of an ileostomy is not without potential serious complications. A high output ileostomy would result in dehydration and electrolyte derangements, leading to a potential allograft failure. In addition, a second surgery for reversal of such ileostomy in the now ‘chronic’ immunosuppressant and steroid use would significantly increase the risk of postoperative anastomotic complications.
It seemed that only one of the three immunsopressants used in our patient was linked to poor colonic anastomosis healing, and this medication (prednisone) was administered at low dose. Given the absence of other comorbidities known to negatively impact wound healing and the potential negative effects on the new allograft function due to complications from an ileostomy, we decided to not proceed with flow diversion.
In conclusion, diagnosis and management of bowel ischemia in the solid organ transplanted patient represents a challenge to the acute care surgeons. Careful consideration must be given to assess the risk of devastating complications following operative intervention in the setting of immunosuppressant therapy, that is, anastomotic leak versus allograft dysfunction, when selecting the operative approach. Fecal diversion may be avoided in the patient with low comorbidities but may be necessary in those with multiple comorbidities. Approach should be left at the surgeon’s discretion. New tools have been developed to assist in calculating the risk for intestinal anastomosis leak which may facilitate operative decision making.
Footnotes
Contributors WAG: involved in the conception of the manuscript and provided critical review. SV-P and CDL: performed the literature review and drafted the manuscript. LKK and WAG: involved in manuscript proof-reading and revisions. All authors provided care for the patient in question.
Competing interests None declared.
Patient consent Not obtained. Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/




{kind=link}
{kind=link}