

Abstract
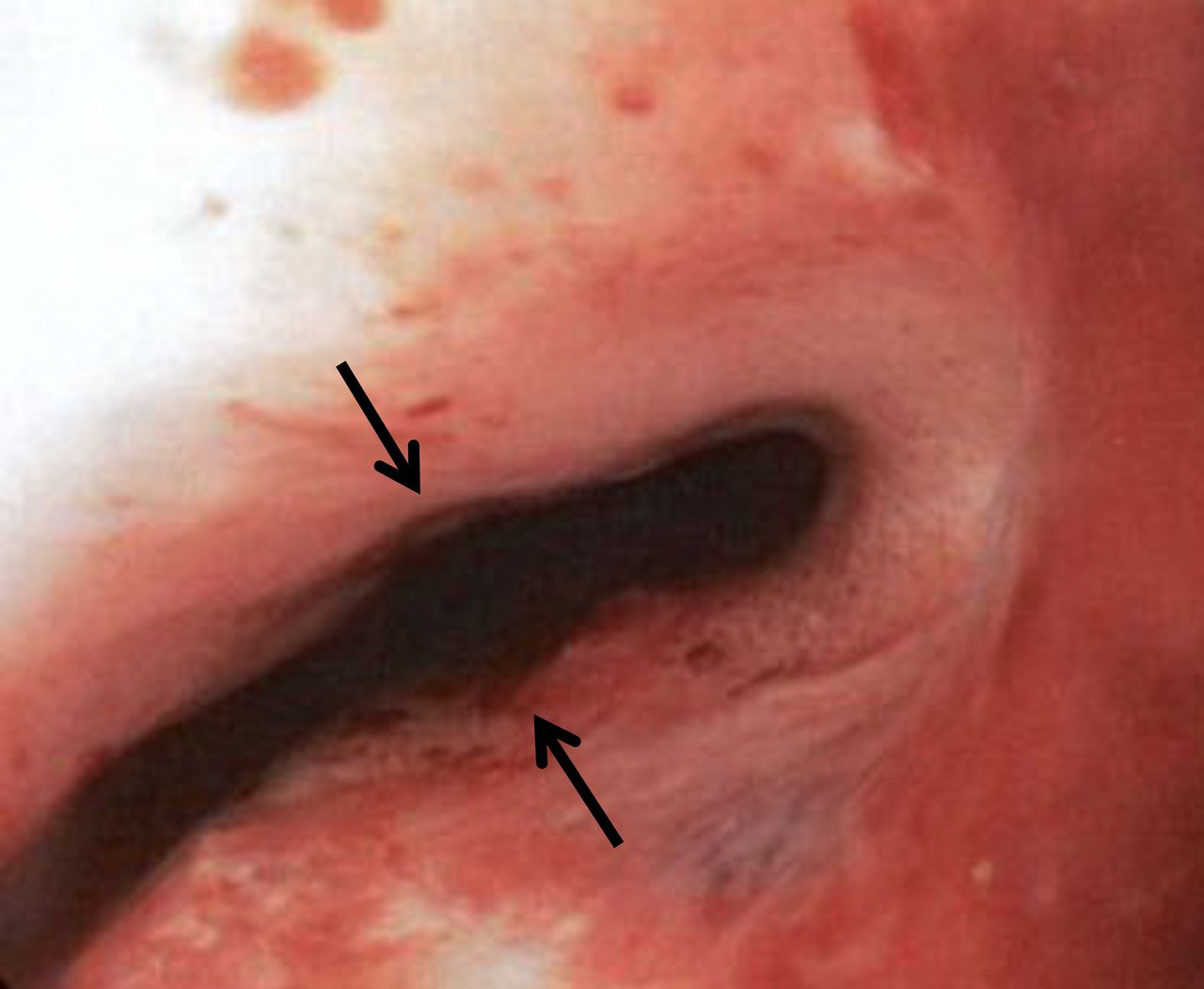
A 42-year-old man presented to the emergency department with gunshot wound to left upper back over the scapula and palpable bullet over the right supraclavicular fossa. The patient had a left-sided needle thoracostomy in the field. He was tachypneic and tachycardiac but normortensive on arrival. Due to the patient being in respiratory distress, he was orotracheally intubated. On examination, he was found to have a moderate left pneumothorax with mild mediastinal shift. He had a left closed tube thoracostomy placed. CT angiography imaging of the neck and chest was then obtained, and pneumomediastinum associated with bony fragmentation of the anterior T1 and T2 vertebral bodies was observed. Additional findings included right internal jugular injury and right apical pulmonary hemorrhage. The patient subsequently underwent flexible tracheobronchoscopy and esophagoscopy in the endoscopy suite, where a through-and-through esophageal injury at 21 cm from the incisors was recognized (figure 1). There was erythema noted in the trachea at this level, but no evidence of transmural injury to the trachea.
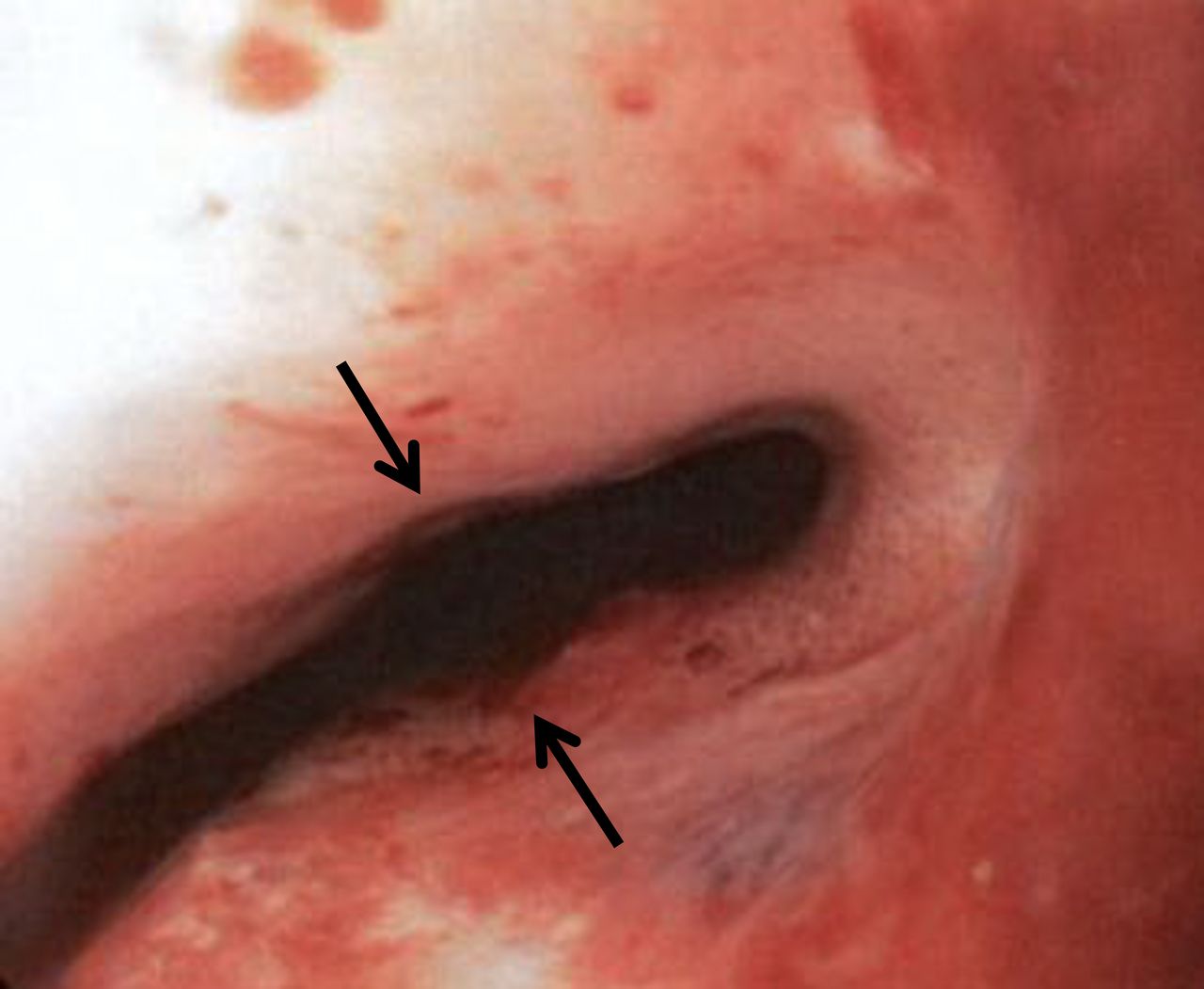
Through-and-through gunshot wound to esophagus. Arrows denote areas of injury.
What would you do?
Commence 14-day course of broad spectrum antibiotics.
Endoscopic stenting with video-assisted thorascopic surgery (VATS) washout.
Local exploration with wide drain placement.
Open esophagectomy with spit fistula.
What we did and why?
Correct answer: B
The patient was taken subsequently to the operating room, and we proceeded with aright-sided VATS. An apical hematoma was identified, and the hematoma was evacuated and underlying pleura was opened. Irrigation was performed and drains were placed. The patient was then placed in supine position, and a 23×100 mm covered esophageal stent was deployed endoscopically, along with nasogastric and nasoenteric feeding tubes (figure 2). The patient was extubated on postoperative day #1 and subsequently kept with nutritional support via nasoenteric tube and continuation of intravenous antibiotics. On postoperative day #5, the patient was taken back to the endoscopy suite for repeat bronchoscopy, which demonstrated intact trachea, and flexible esophagoscopy was performed along with repositioning of the stent under fluoroscopy due to distal migration of the stent.

Esophageal stent covering area of injury.
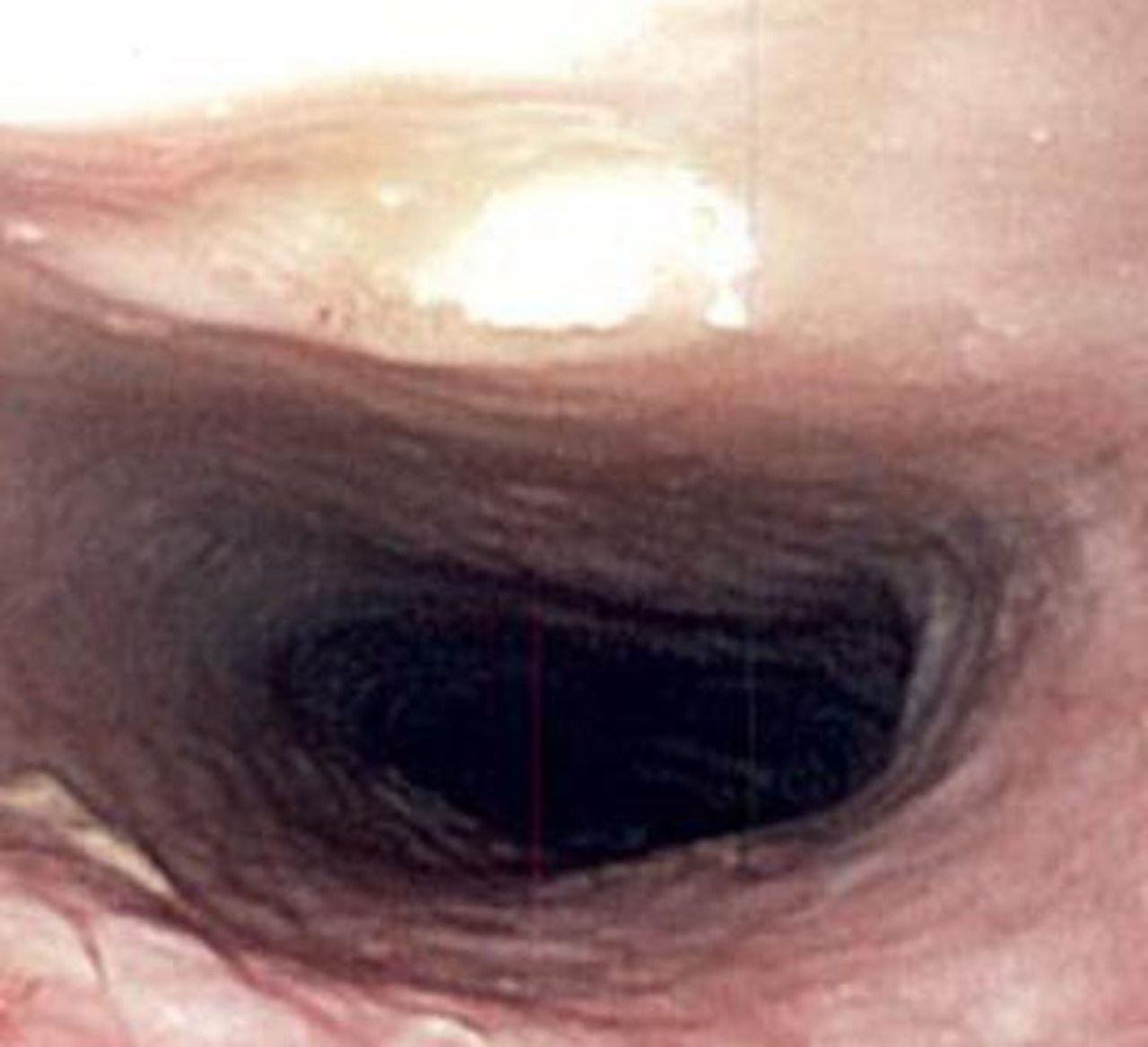
Repeat esophagoscopy was performed on post-trauma day #10 for consideration of stent removal, but it was observed that the gunshot wound had not satisfactorily healed, and the indwelling stent was causing some erosion of the esophageal mucosa. The stent was therefore replaced. Repeat endoscopy was performed on post-trauma day #14, and it was determined that the esophageal gunshot wounds had sufficiently healed and the stent was able to be removed (figure 3). The patient was subsequently discharged home after commencing oral intake.
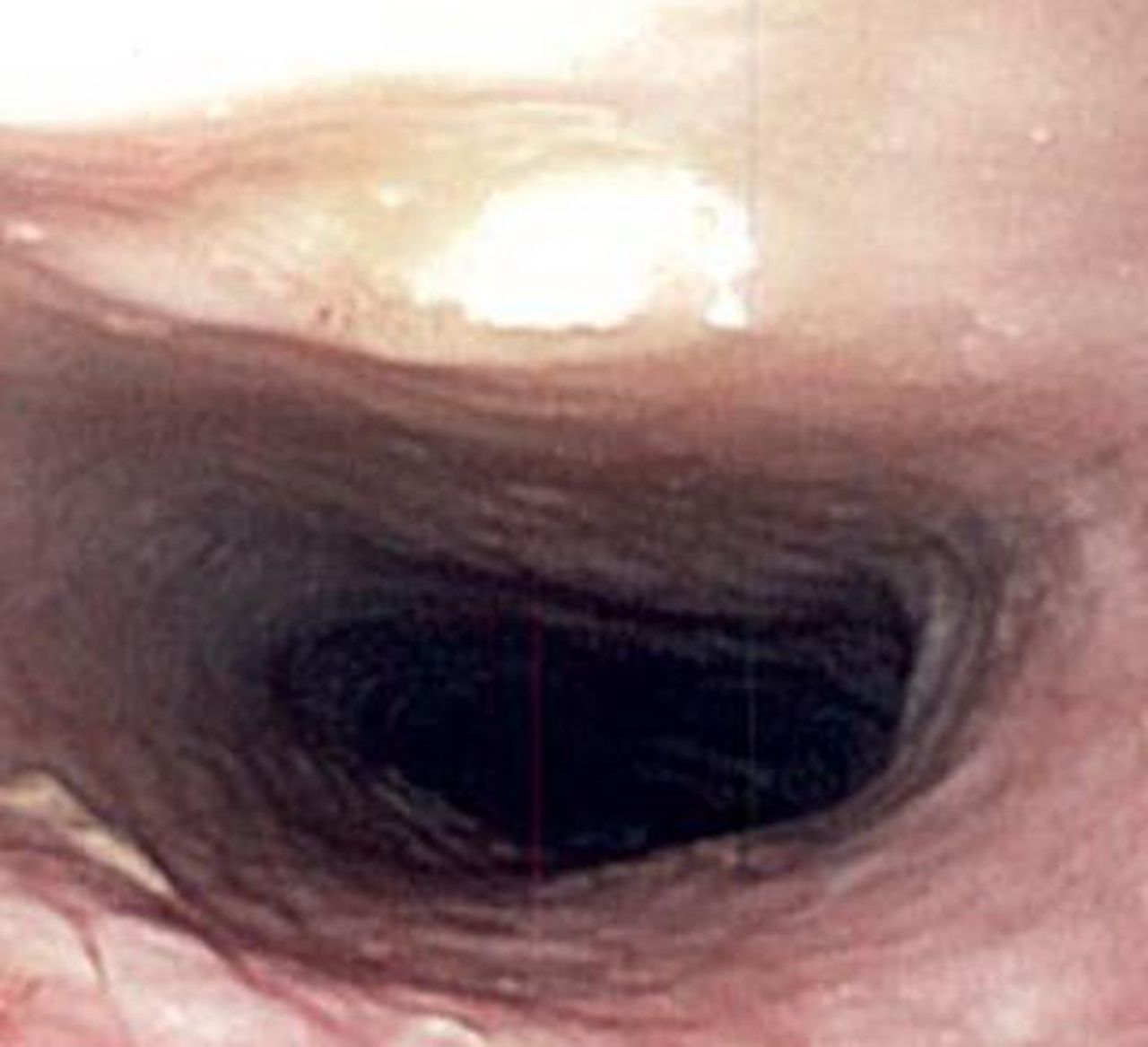
Endoscopy following stent removal 2 weeks following injury demonstrating healed mucosa.
Penetrating injury to the esophagus is encountered with relative infrequency and remains among the most challenging of wounds to manage while avoiding major postoperative morbidity. While early operative repair offers the best opportunity for success, it relies on sufficient exposure that may be technically difficult to achieve. In addition, although aggressive esophageal mobilization may improve exposure of the wound(s) requiring repair, such a maneuver may risk injury to the esophageal blood supply, resulting in devascularization. When situated at the thoracic inlet, injury to the esophagus is particularly troublesome as neither the cervical nor thoracic approach to the wound is particularly gratifying given the limited space in which to expose the injury.
Non-operative management may be considered for small contained leaks, but a through-and-through gunshot wound is often not suited for a non-operative approach. However, within the last decade, advances in endoscopic and minimally invasive techniques have demonstrated the efficacy of endoscopically placed stents in the management of nontraumatic esophageal conditions, namely spontaneous perforations, anastomotic leaks, and iatrogenic injury. Temporary stent placement by endoscopic technique has been effective for patients with large esophageal leaks and is associated with an overall success rate of 81%–91% and low incidence of serious complications.
Commentary
This case highlights the potential benefit of endoscopic stent placement for definitive management of penetrating esophageal trauma. For this patient, a difficult and potentially morbid surgical exposure of this thoracic inlet injury was avoided, and the not uncommon morbidity of suture line breakdown and esophageal-cutaneous fistula was thereby avoided as well. As experience with endoscopic stent placement continues to accrue, it is imaginable that this relatively less invasive modality may become a first-line management modality for traumatic esophageal injuries.
Footnotes
Contributor NSR, SI, JLS and VAG contributed to manuscript preparation. KPM, JAW and RMB contributed to critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0




{kind=link}
{kind=link}
{kind=link}