

Abstract
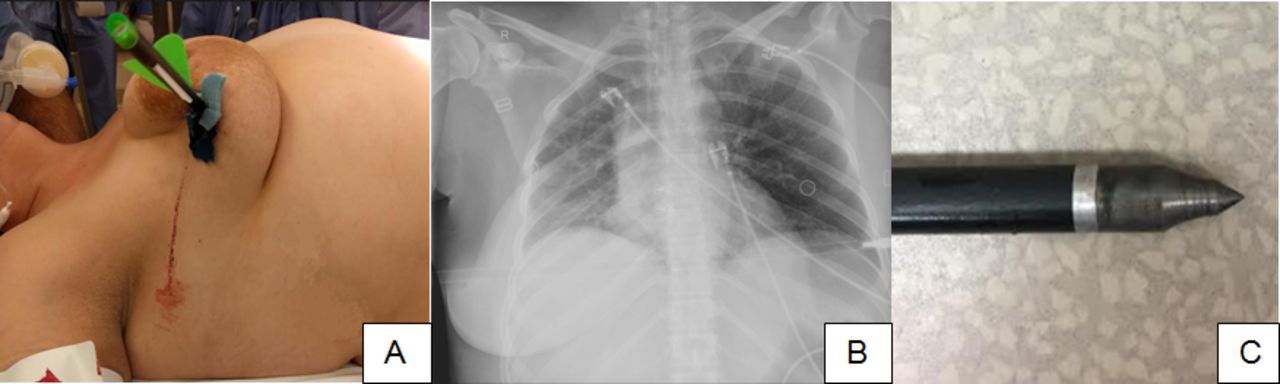
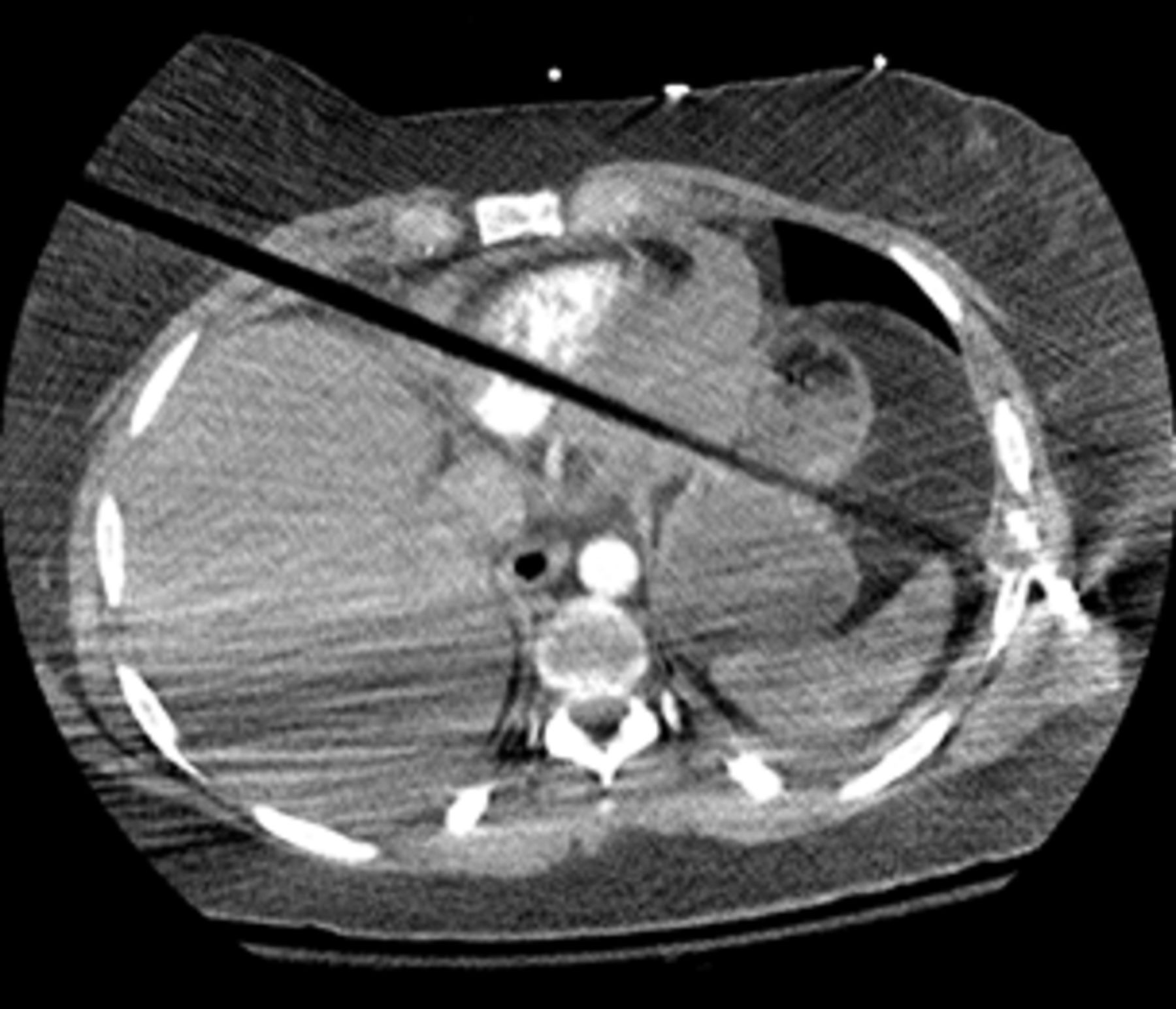
Case summary A 33-year-old woman was transferred from an outside hospital with a penetrating injury to her right chest. The patient was shot with a crossbow with the entry site to the right breast/chest and a transmediastinal trajectory. She was intubated prior to arrival due to difficulty breathing. Her vital signs remained stable and within normal limits, with good breath sounds, and no evidence of pneumothorax on chest X-ray. The tip of the bolt was palpable at the patient’s left midaxillary line. Chest X-ray in trauma bay showed the transmediastinal trajectory, and the bolt appeared to have a field point (not a broadhead point) (figure 1). A CT of the chest was obtained to assist with surgical planning. Images showed the bolt penetrating the right chest, right ventricle and inferior aspect of the left ventricular muscle, through the stomach, and ending near the tip of the spleen with a fracture of the left seventh rib (figure 2).

Image A shows the bolt (crossbow arrow) entering the patient’s right breast and chest. Image B is the chest X-ray taken in the trauma bay showing the transmediastinal trajectory and partial visualization of the tip of the bolt with a field point. Image C demonstrates the tip of the bolt after removal.
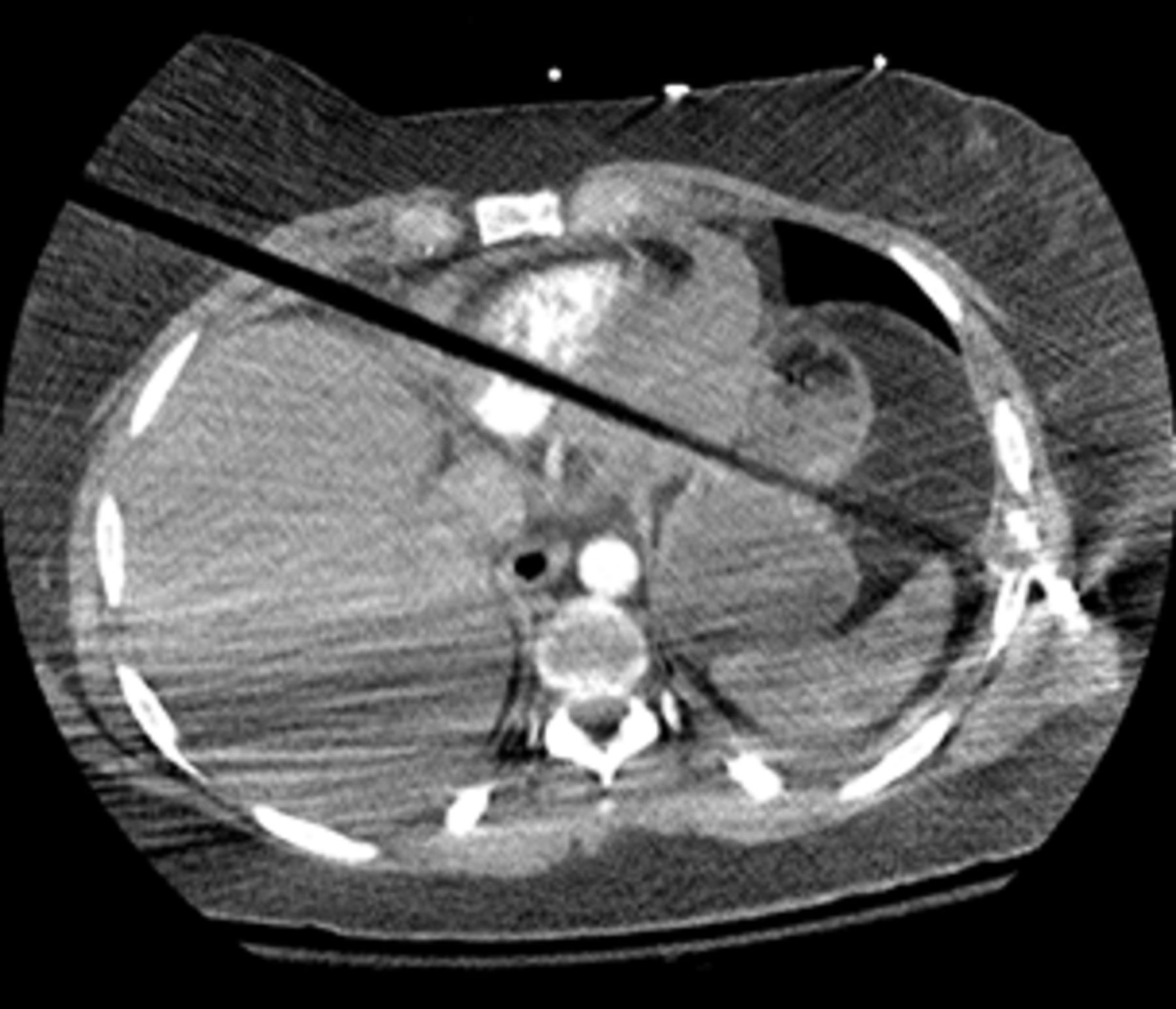
CT of the chest with intravenous contrast showing a foreign body penetrating the right chest at the fourth intercostal space, right ventricle, left ventricle muscle, left hemidiaphragm, through the stomach, and ending near the tip of the spleen without injury to it. There was also a fracture of the lateral seventh rib and hemopericardium. The tip of the bolt is not clearly demonstrated due to artifact.
What would you do?
Median sternotomy followed by midline laparotomy.
Clamshell thoracotomy in the Emergency Room (ER).
Right anterolateral thoracotomy.
Left posterolateral thoracotomy.
What we did and why
The correct answer is A. The patient remained hemodynamically stable in the trauma bay. A CT of the chest was obtained to assist with surgical planning. Images showed the bolt penetrating the right chest, right ventricle and inferior aspect of the left ventricular muscle, through the stomach, and ending near the tip of the spleen with a fracture of the left seventh rib (figure 2).
Cardiothoracic surgery was consulted for assistance. The patient was taken to the operating room (OR). In the OR, a transesophageal echocardiogram was performed, which demonstrated the bolt penetrating the cardiac musculature, but not entering any chamber. A significant pericardial effusion was also demonstrated along with limited mobility of the heart due to it being “pinned down.”
A median sternotomy was performed and the pericardial tamponade was released. The bolt had penetrated the anterior right ventricular wall and exited posteriorly. The patient was placed on cardiopulmonary bypass and the heart decompressed. The bolt was carefully removed and both holes were repaired with pledgeted sutures. The defect in the left hemidiaphragm was also repaired. Drains were placed in the pericardial sac and both pleural cavities. She remained hemodynamically stable during most of the case. A midline laparotomy was performed and the two gastrostomies in the proximal stomach were repaired. The spleen was uninjured and there were no other intra-abdominal injuries. Her postoperative course was uncomplicated and she was discharged home on postoperative day 7.
Deciding factors for the type of incision and exposure include mechanism, trajectory, number of penetrating missiles, and known and anticipated injuries. Preoperatively in this case, cardiac, diaphragmatic, and gastric injuries were recognized. The development of a cardiac tamponade was anticipated and the degree of bilateral lung injury was uncertain. The chest X-ray showed no evidence of hemothorax or pneumothorax. These factors, including the potential for cardiopulmonary bypass, led to the decision to use a median sternotomy for the optimal exposure for the cardiac injury. Left posterolateral thoracotomy may have provided good exposure for the lateral posterior cardiac injury, but not optimal for cardiopulmonary bypass. Cardiopulmonary bypass was selected to be used for this case and aided with the repair of the injury in a stress-free fashion. The patient did well and attained, full recovery and returned to her activities of daily living.
Footnotes
Contributors DJ and PE had equal contribution to this article.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}