

Abstract
Background A growing body of research has explored patient satisfaction as one of the healthcare quality measures. To date, scarce data are available regarding family experience in the trauma and surgical intensive care unit (TSICU). The purpose of this study was to describe and analyze the results of a family satisfaction survey in the TSICU.
Methods Family members of patients at a level 1 trauma center were invited to participate in this study after 72 hours of intensive care unit stay. Participants completed a modified version of the Family Satisfaction in the Intensive Care Unit questionnaire, a validated survey measuring family satisfaction with care and decision-making. Data collection spanned from April 2016 to July 2017. Patient characteristics were compiled from the medical record. Quantitative analysis was performed using a 5-point Likert score, converted to a scale of 0 (poor) to 100 (excellent).
Results The overall response rate was 78.6%. Of the 103 family members for 88 patients, most were young (median age: 41 years) and female (75%). Language fluency was 44.6% English-only, 31.7% Spanish-only, and 23.8% bilingual. Mean summary family satisfaction scores (±SD) were 80.6±26.4 for satisfaction with care, 79.3±27.1 for satisfaction with decision-making, and 80.1±26.7 for total satisfaction. Respondents were less satisfied with the frequency of communication with physicians (70.7±27.4) and language translation (73.2±31.2).
Discussion Overall family satisfaction with the care provided to patients in the TSICU is high, although opportunities for improvement were noted in the frequency of communication between physicians and family and language translation services. Further quality improvement projects are warranted.
Level of evidence Care management study: level V.
Introduction
Medicine is a field of continual progress, spurred on by innovation and constantly seeking to improve itself. Beyond the technological advances and scientific breakthroughs that have shaped the standard of care, a fundamental shift in the definition of quality healthcare arrived with the release of the Institute of Medicine’s report, Crossing the Quality Chasm: A New Health System for the 21st Century.1 Among the six key areas for improvement detailed in this report is patient-centered care, defined as “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.”1 Indeed, hospitals are now required to demonstrate higher quality, patient-centered care at a lower cost, in addition to conventional outcome measures such as mortality rate, complication rate, and length of hospital stay.2 Thus, a growing body of research has explored patient satisfaction as one of the healthcare quality measures.3 4 Recent literature has shown that high patient satisfaction is correlated with higher surgical quality and efficiency of care as well as low mortality.5 6 However, in the trauma and surgical intensive care unit (TSICU), patients are critically ill and may be unable to participate in decisions regarding their care, often leaving family members to take on the role of surrogate decision-maker.7 8
In recent years, several types of survey tools have been developed and used to better assess family satisfaction as a proxy for measuring the quality of healthcare in the intensive care unit (ICU).9–13 One of them is the Family Satisfaction in the Intensive Care Unit (FS-ICU), a validated questionnaire developed by the Canadian Researchers at the End of Life Network in 2003 and revised in 2006.10 11 Studies using the FS-ICU tool have demonstrated that family satisfaction in the ICU is consistently high in adults, children, and Hispanic populations.14–17 Data remain scarce on the utility of the FS-ICU to evaluate the level of family satisfaction in the TSICU. As for other types of ICU patients, family is a key component of the healing team for critically ill trauma and surgical patients. It may follow that a highly satisfied family member will be better prepared to provide support for their loved one, participate in the decision-making process, and perhaps positively influence patient care. The purpose of this study was to describe and analyze the results of a family satisfaction survey conducted in the TSICU. We developed two hypotheses for this study: first, that it would be feasible to conduct a family satisfaction study in the TSICU using a largely prevalidated survey, and second that the survey could identify areas for improvement in patient care within the study facility.
Methods
Study design and population
This was a prospective observational study conducted from April 2016 to July 2017. Patients admitted to one of four acute care surgery services in the TSICU and their family members at LAC+USC Medical Center, a level 1 trauma center, were invited to participate in this study by research personnel after 72 hours of ICU stay. After eligible patients and their family (≥18 years old) were identified, research personnel provided information about the study and distributed the survey. Subjects were informed that their participation was voluntary, their responses would not be seen by the patient’s care providers, and participation in this study would have no direct impact on their loved one’s care. Only family members fluent in English or Spanish were approached for the study, with those fluent in both languages given the option of completing either version of the questionnaire. Survey recipients were instructed to complete the form at their convenience and return the questionnaire. If applicable, multiple family members were given the opportunity to complete the survey form for each patient.
Survey instrument
The FS-ICU 24 is a validated survey measuring family satisfaction in the domains of satisfaction with care (14 items) and decision-making (10 items).11 In addition to these 24 scored items, the survey includes a brief demographics section and three short-answer questions for participant comments. The FS-ICU 24 was modified for this study to include eight additional items on satisfaction with hospital food, translation services, hospital visiting times, and interactions with ancillary staff. Although these supplementary questions had not been previously validated, they were included as baseline metrics of the TSICU’s performance beyond that provided by the original FS-ICU 24. The instrument was made available to study participants in English and Spanish (online supplementary file 1 and 2).
Data collection and statistical analysis
The results of the modified FS-ICU 24 were compiled in a secure web application system, REDCap (Research Electronic Data Capture). Quantitative analysis of the FS-ICU was performed using a 5-point Likert score, converted to a scale of 0 (poor) to 100 (excellent), as described previously.10 The average score and SD were computed for each variable, as well as summary scores for satisfaction with care (FS-ICU/Care), satisfaction with decision-making (FS-ICU/DM), and total composite score (FS-ICU/Total).11
Results
During a 15-month study period, a total of 2150 patients were admitted to the TSICU. Of 131 family members approached, 103 family members submitted questionnaires for 88 patients (response rate: 78.6%). Eighty-seven out of 103 surveys (84.5%) were completed by family members of the 74 trauma patients enrolled in this study. Among the cohort of trauma patients, 66 patients had one family survey respondent, 5 patients had two respondents, 2 patients had three respondents, and 1 patient had five respondents. Sixteen surveys were completed by family members of 14 patients admitted for the management of emergency general surgery disorders; 13 patients each had one survey respondent, whereas 1 patient had three submissions. The median age of study patients was 37.5 years and 71.6% were male. Of 74 trauma patients, 83.7% sustained blunt injuries. Overall, inmortality rate was 6.8% and the median ICU stay was 11 days. Family respondents were mostly young (median age 41, IQR 29–56) and female (75%). Forty-five percent had been involved as family of an ICU patient in the past, and 60.8% reported living with the patient. Language fluency was 44.6% English-only, 31.7% Spanish-only, and 23.8% bilingual.
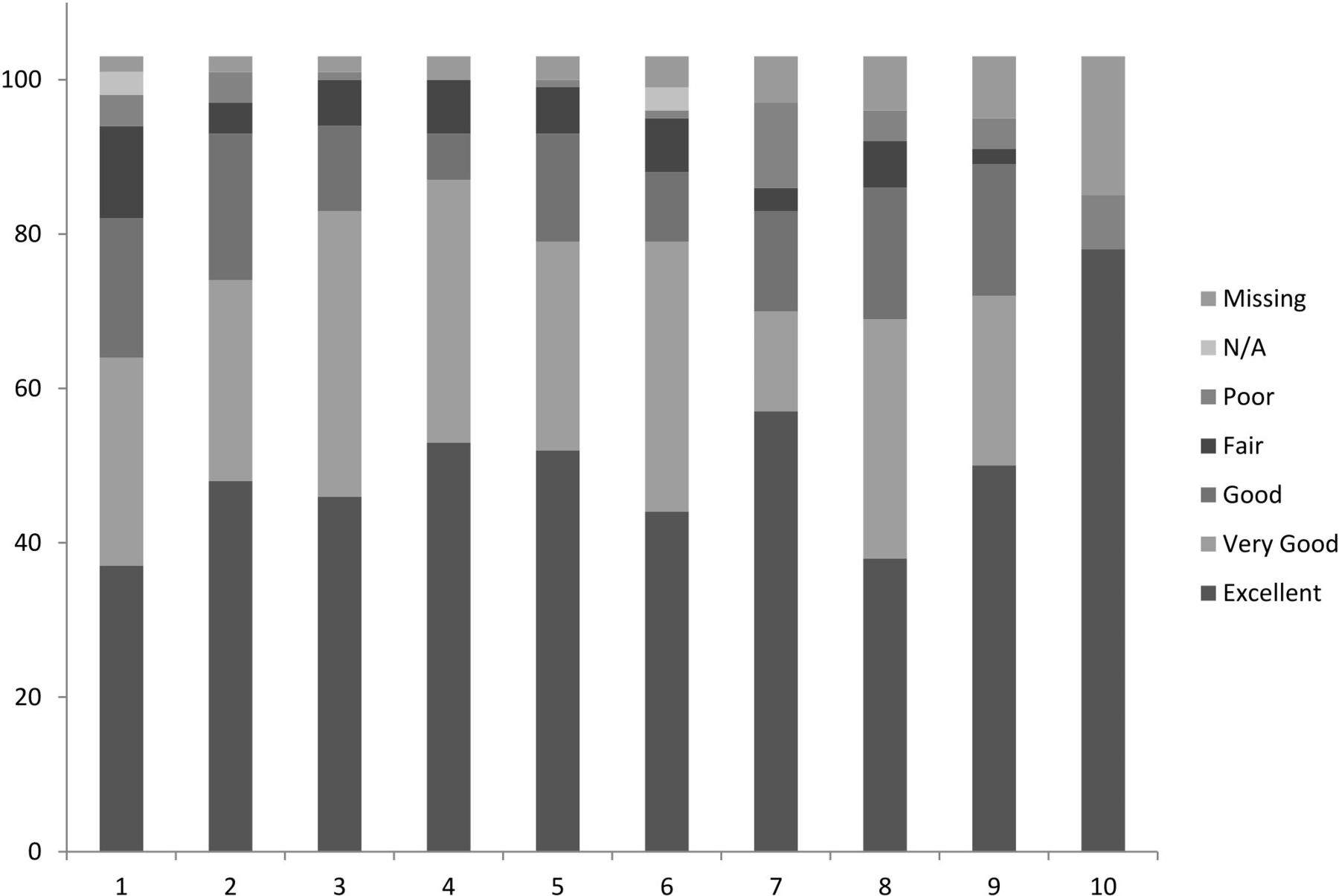
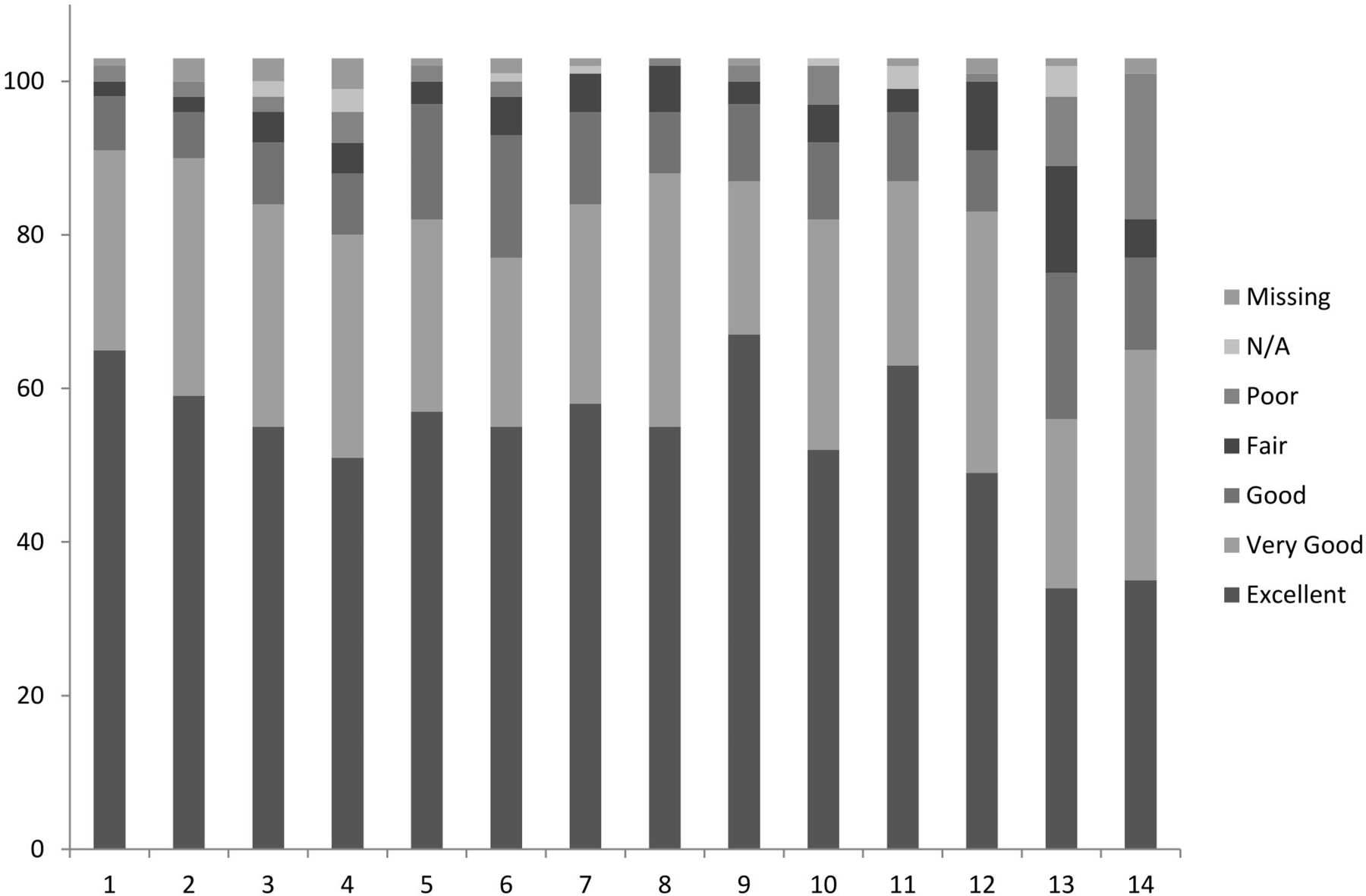
Summary family satisfaction scores were calculated for the standardized FS-ICU 24 items. The mean scores (±SD) were 80.6±26.4 for FS-ICU/Care, 79.3±27.1 for FS-ICU/DM, and 80.1±26.7 for FS-ICU/Total. Response distribution for each survey item is shown in figures 1 and 2. Individual items earning the highest scores were satisfaction with the amount of time to make decisions and ask questions (91.8±27.5), the skill and competence of ICU doctors (87.1±19.6) and nurses (86.0±23.1), and satisfaction with the concern and caring by the ICU staff for the patient (86.8±21.5) and pain management (85.8±21.3). Conversely, lowest scoring items were satisfaction with the level or amount of care provided (64.1±36.8), the atmosphere of the waiting room (64.8±33.3), and the frequency of communication with doctors (70.7±29.5) (tables 1 and 2).

Family satisfaction with care response distribution (number of responses). (1) Concern and caring by the ICU staff for the patient. (2) Symptom management: pain. (3) Symptom management: breathlessness. (4) Symptom management: agitation. (5) How well the ICU staff showed an interest in family member’s needs. (6) How well the ICU staff provided emotional support. (7) The teamwork of all the ICU staff who took care of the patient. (8) The courtesy, respect, and compassion given to family member. (9) How well the nurses cared for the patient. (10) How often the nurses communicated with family member about the patient’s condition. (11) How well doctors cared for the patient. (12) Atmosphere of the ICU. (13) Atmosphere of the ICU waiting room. (14) How satisfied was the family member with the level or amount of care received by the patient. ICU, intensive care unit; N/A, not applicable.
Family satisfaction with decision-making response distribution (number of responses). (1) How often doctors communicated with family member about the patient’s condition. (2) Willingness of the ICU staff to answer questions. (3) How well the ICU staff provided explanations that were easy to understand. (4) Honesty of information provided to family members about the patient’s condition. (5) How well the ICU staff informed family member of what was happening to the patient and why things were being done. (6) Consistency of information provided about the patient’s condition. (7) Family member inclusion in the decision-making process. (8) Family member support during the decision-making process. (9) Family member feeling of control over the patient’s care. (10) Adequate time to have questions answered. ICU, intensive care unit; N/A, not applicable.
Family satisfaction with care scores
Family satisfaction with decision-making scores
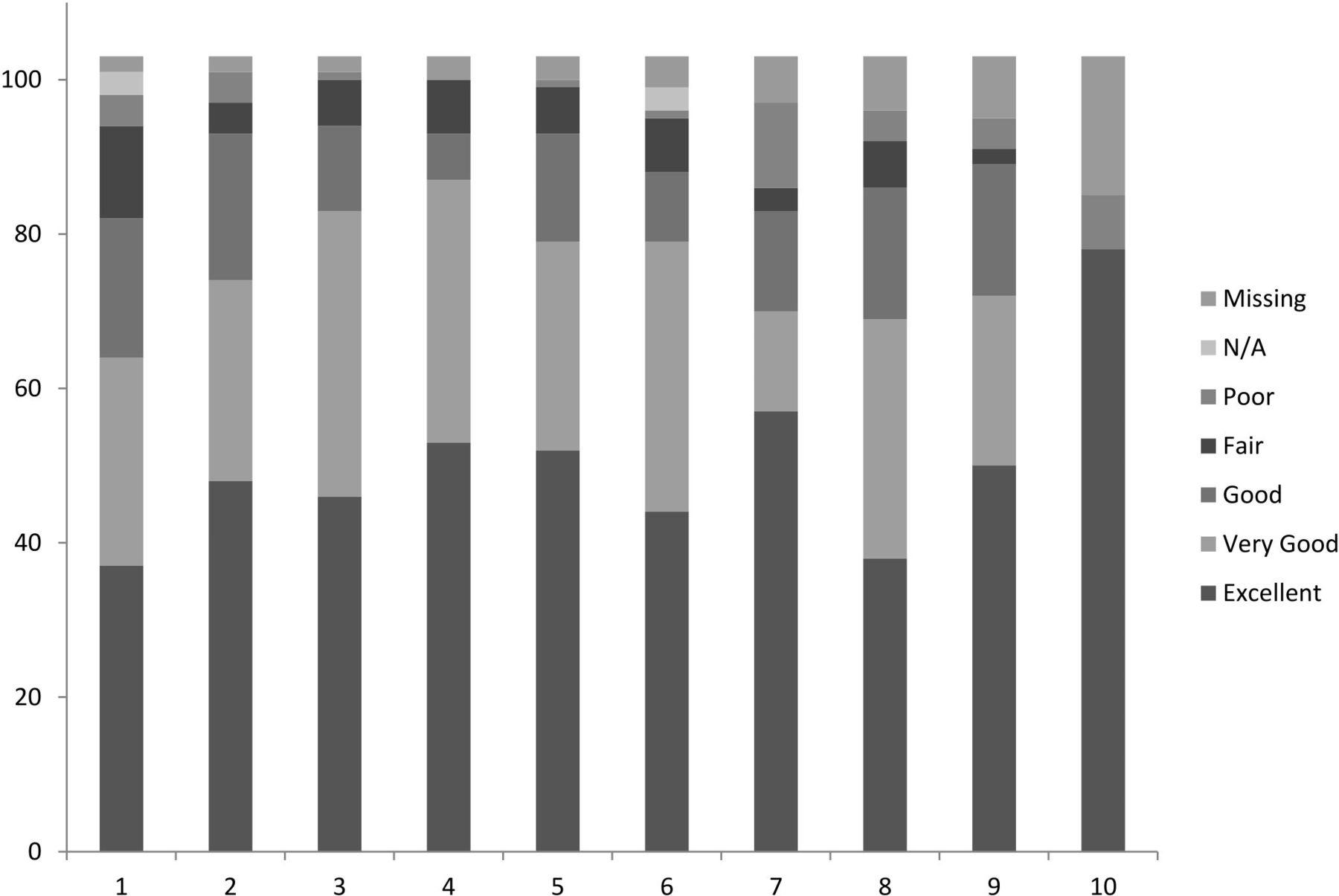
Eight supplementary items were also evaluated in this survey, and the response distribution is shown in figure 3. Family members were highly satisfied with the hospital policy on waiting times (85.9±21.1), less satisfied with social work (69.7±30.0) and spiritual services (69.4±29.0), and least satisfied with the quality of hospital food for patients (51.4±31.8) and family (60.1±30.7) (table 3). Seventy-six of 103 participants submitted qualitative responses, which were largely positive and reflective of the scored items on the survey. Several participants expressed gratitude to the medical staff and endorsed high satisfaction with the quality of care in the TSICU. Among the negative comments, multiple responses called for improvements with the comfort/amenities of the waiting room and sleeping conditions for family members, more frequent communication with physicians, and a desire for more bilingual (English-speaking and Spanish-speaking) staff.

Supplementary satisfaction items response distribution (number of responses). (1) Patient’s satisfaction with hospital food. (2) Family member satisfaction with hospital food. (3) Language translation services. (4) How language barriers between ICU care providers and the patient were handled. (5) Spiritual support services at the hospital. (6) Social work services provided to the patient and/or family member. (7) Patient’s interaction with ancillary staff. (8) Hospital’s policy regarding visiting times. ICU, intensive care unit; N/A, not applicable.
Supplementary item family satisfaction scores
Discussion
In this study, we sought to characterize family satisfaction in the ICU in a population composed primarily of trauma and emergency general surgery patients. Our response rate of 78.6% was within the range of 27.8% to 84.0% reported in previous publications, supporting the hypothesis that a family satisfaction survey is feasible in the TSICU.14 17 Our results demonstrate that overall family satisfaction in the TSICU is high; the three summary satisfaction scores derived from our survey instrument were all approximately 80 out of a possible 100 points, translating to a score between very good and excellent satisfaction. These results offer reassurance of the high-quality care provided at our facility. Respondents acknowledged the skill of our providers and their ability to manage patients’ symptoms, as these questions were among the highest-scoring items on the survey instrument. However, the results also present opportunities to address items with lower satisfaction; the frequency of family communication with physicians, the quality of language translation services, and the comfort and amenities of the family waiting room are all candidates for improvement.
The results presented here are comparable with those of prior studies using the FS-ICU survey instrument. Lam et al15 collected the FS-ICU questionnaire from 736 family members at a medical-surgical ICU in Hong Kong, and obtained summary satisfaction scores of 78.0±16.8 for FS-ICU/Care, 78.6±13.6 for FS-ICU/DM, and 78.1±14.3 for FS-ICU/Total. Another study investigated family satisfaction at four ICUs in Germany, receiving 215 completed surveys and finding summary scores of 78.6±14.3 for FS-ICU/Care, 77.8±15.6 for FS-ICU/DM, and 78.33±14.30 for FS-ICU/Total.14 Similarly, Stricker et al performed a multicenter study of Swiss ICUs, analyzing 996 surveys and finding summary scores of 79±14 for FS-ICU/Care, 77±15 for FS-ICU/DM, and 78±14 for FS/ICU-Total.18 A notable difference between our study and previous work is evident in the patient population; whereas others identified patients exclusively in the medical ICU (MICU) or ICU patients with a diverse range of medical, surgical, cardiologic, or neurologic problems, the present study selected almost entirely trauma and emergency general surgery patients. Patients in the MICU are often elderly and suffering from chronic illness, so their hospital course may not be entirely unexpected by family members. Conversely, patients in the TSICU are frequently young, previously healthy individuals, and their sudden hospitalization may place a tremendous acute burden on family decision-makers. We surmise that this may have influenced the role that family members played in the decision-making process.
We think that the results of a family survey which covers several different aspects of patient care in the ICU can be useful in initiating the quality improvement processes as a next step. Our results suggested that there would be opportunities for improvement in communicating with family members, involving them in decision-making processes, and providing translation services. In fact, shortly after the results of our survey were shared with members in the multidisciplinary TSICU care team, we developed several quality improvement projects for each item with a lower satisfaction score. For example, we have created a protocol in organizing a family meeting within 72 hours after ICU admission to discuss the goals of care in elderly patients with severe traumatic brain injury. In addition to the TSICU team, nursing staff, social workers, other surgical services (eg, neurosurgery, orthopedic surgery), and palliative care team are participants in the meeting. Although it is not always possible to schedule the meeting early in the patient’s hospital stay due to the unique characteristics of our patient population, a postintervention survey is planned, with the hope of observing a significant improvement in family satisfaction.
There are several limitations to this study. First, our results may not reflect the overall population of patients and family members in the TSICU as we used a sample of convenience; the only patients recruited into this study were those who had family at their bedside or in the waiting room. Additionally, we were unable to compare family demographics between respondents and non-respondents. Despite this sampling limitation, the patient demographics and outcomes in the current study were comparable with those from previous studies in our TSICU.19 20 Although conducting telephone or mail surveys might have been alternative methods, we thought that it would not be feasible to conduct those kinds of surveys due to patient characteristics at our institution.3 5 Second, the respondents submitted their response while the patients were still in the TSICU. Although we conducted an anonymous survey, respondents might have felt pressure to respond affirmatively for fear of retribution. Further, the level of family satisfaction can change from admission to discharge of the patient, and the responses we received from family members may not represent overall satisfaction for the entire hospital stay. However, we did not distribute surveys during the postdischarge period, as the aim of this study was to determine the level of family satisfaction with patient care during their ICU stay.
Conclusions
It is feasible to conduct a family satisfaction survey in the TSICU. The modified FS-ICU survey tool can also be administered to family members of patients with critical care conditions managed in the TSICU. Our results suggest that family members were overall satisfied with the care provided in the TSICU. Nonetheless, the survey results were useful to identify opportunities for improvement in patient care and subsequently develop quality improvement programs.
Supplementary data
Supplementary data
Footnotes
Presented at This article was presented at the 13th Annual Academic Surgical Congress in Jacksonville, Florida, January 31, 2018.
Contributors Study concept and design: TM, AA, YH, DA, CM, AS, CP, KM. Data collection and analysis: TM, KM, AA, YH, DA. Article writing: TM, CP, KM. Critical revision: AA, YH, DA, CM, AS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Institutional Review Board at the University of Southern California granted approval for all activities performed in this study.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}