

Article Figures & Data
Figures
- Figure 1
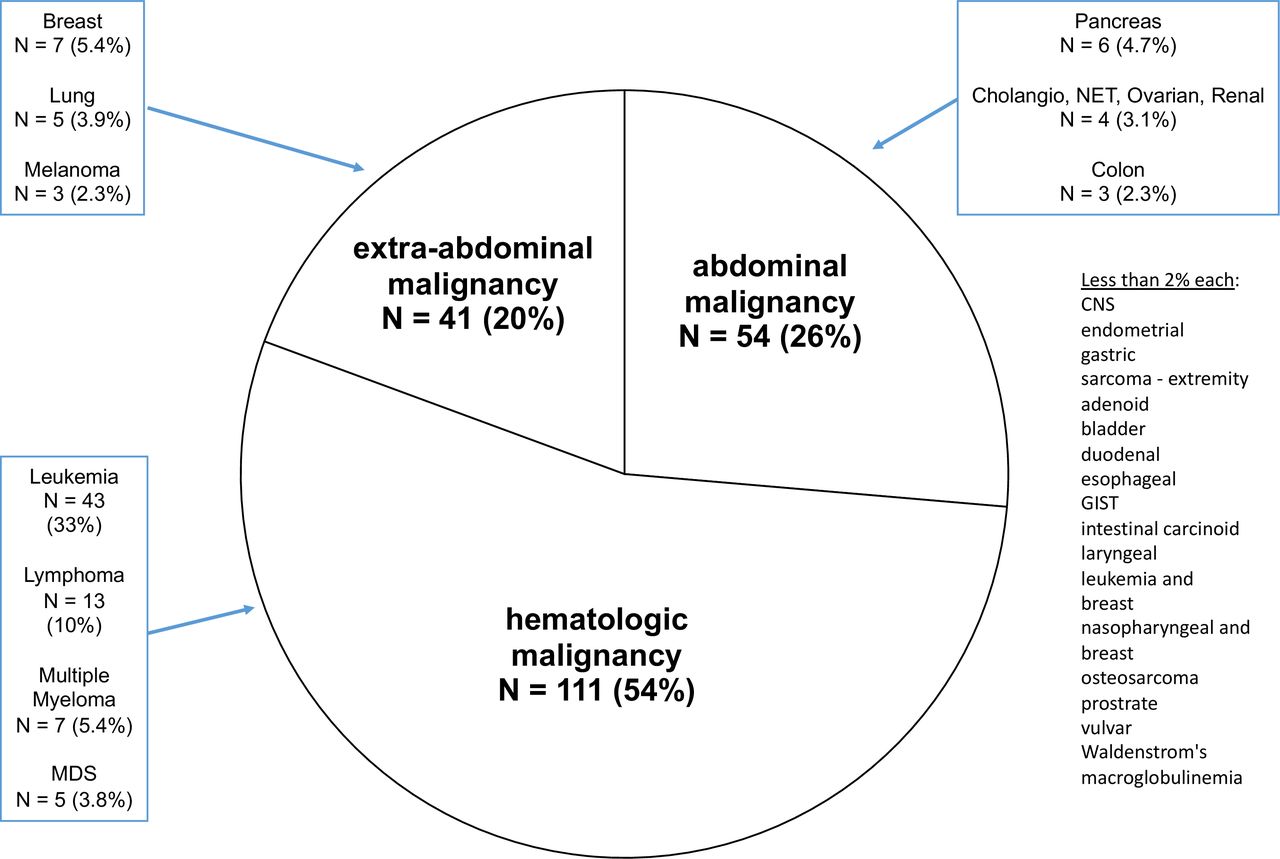
Description of study population by underlying cancer diagnosis. Cancers making up less than 2% of the population: CNS, endometrial, gastric, sarcoma, adenoid, bladder, duodenal, esophageal, GIST, intestinal carcinoid, laryngeal, nasopharyngeal, osteosarcoma, prostrate, vulvar, Waldenstrom's macroglobulinemia. CNS, central nervous system; GIST, gastrointestinal stromal tumor; MDS, myelodysplastic syndrome; NET, neuroendocrine tumor.
- Figure 2
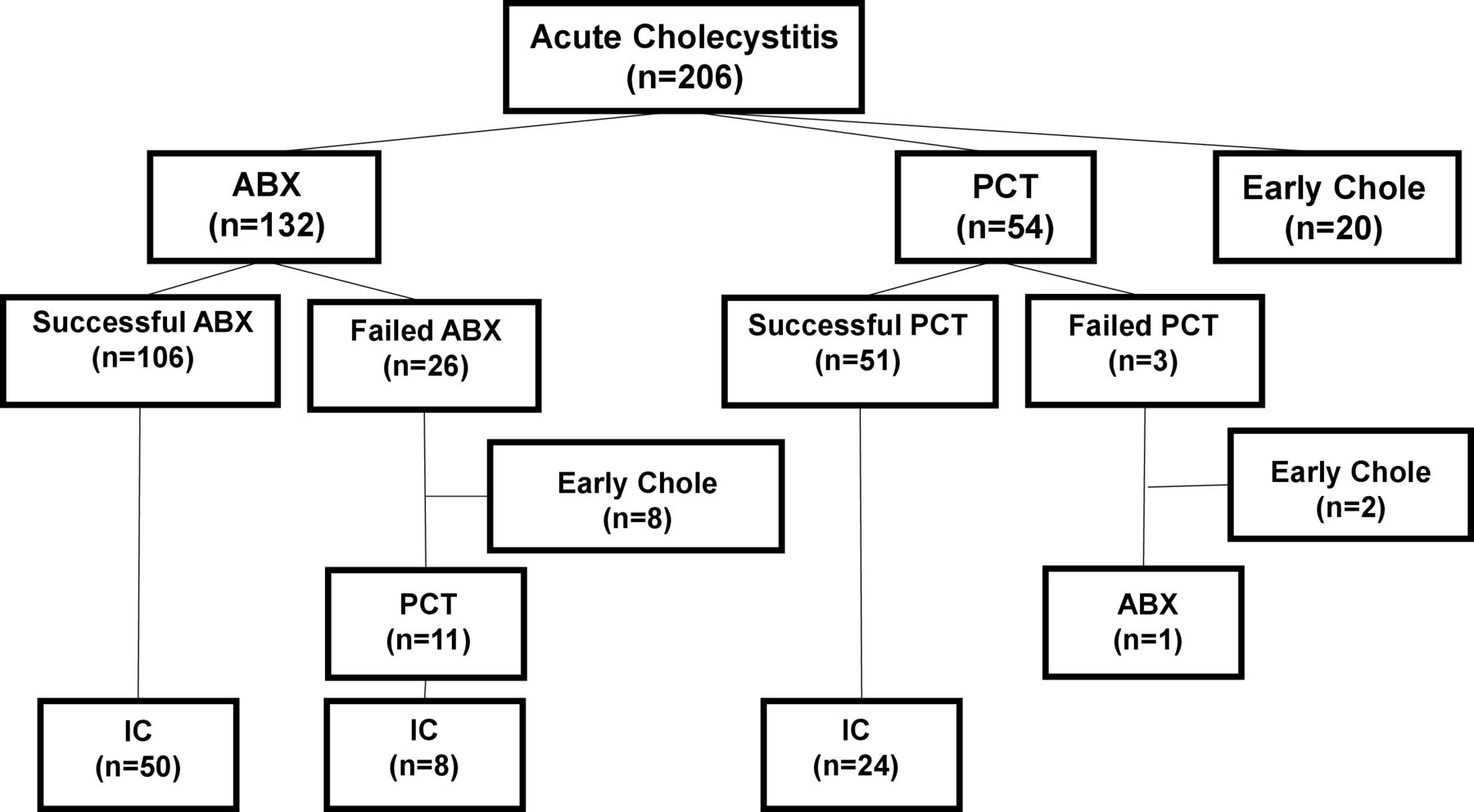
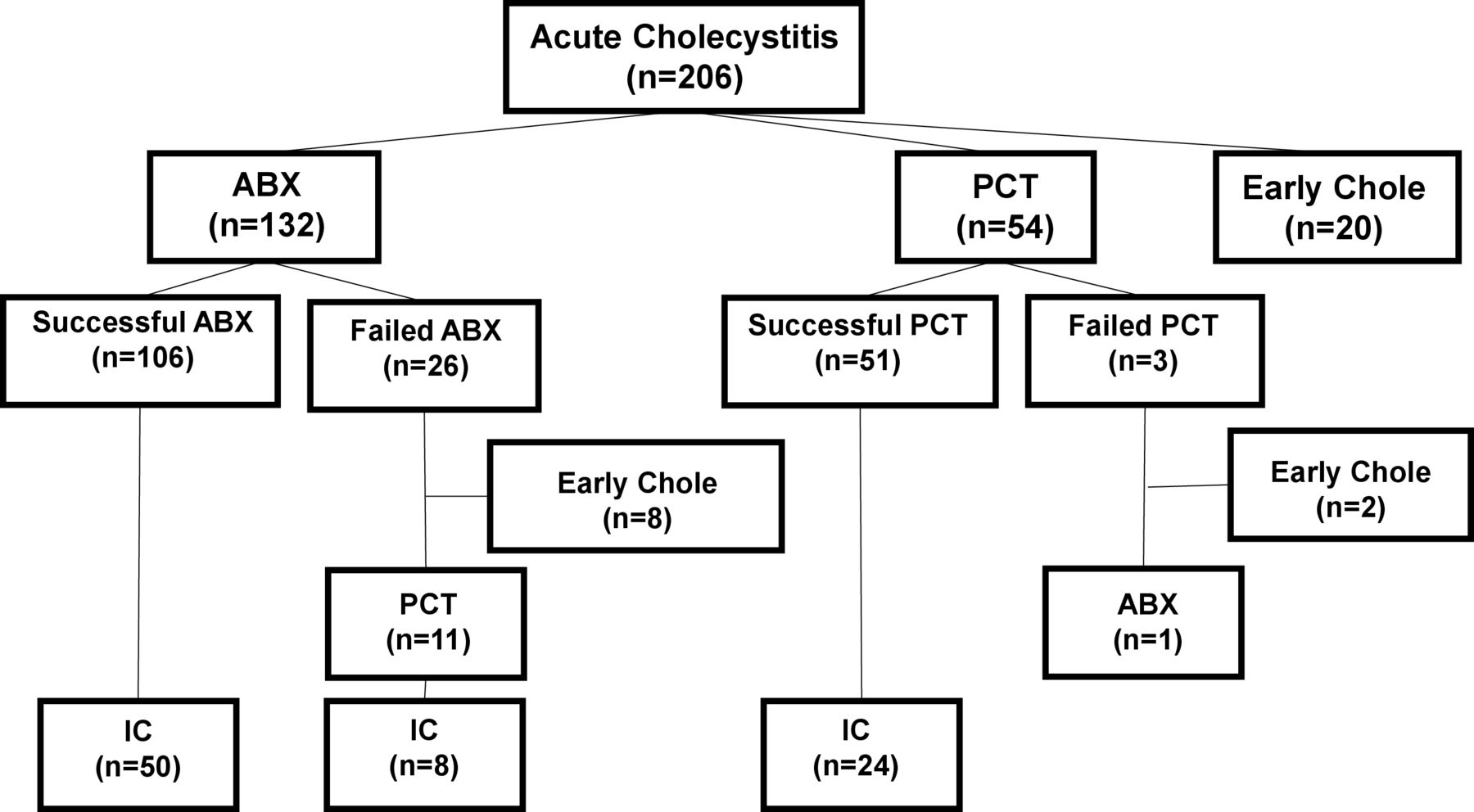
Non-randomized assignment of patients to surgical and non-surgical treatments for acute cholecystitis. legend: ABX, antibiotics; Chole, cholecystectomy; IC, interval cholecystectomy; PCT, percutaneous cholecystostomy tube.
- Figure 3
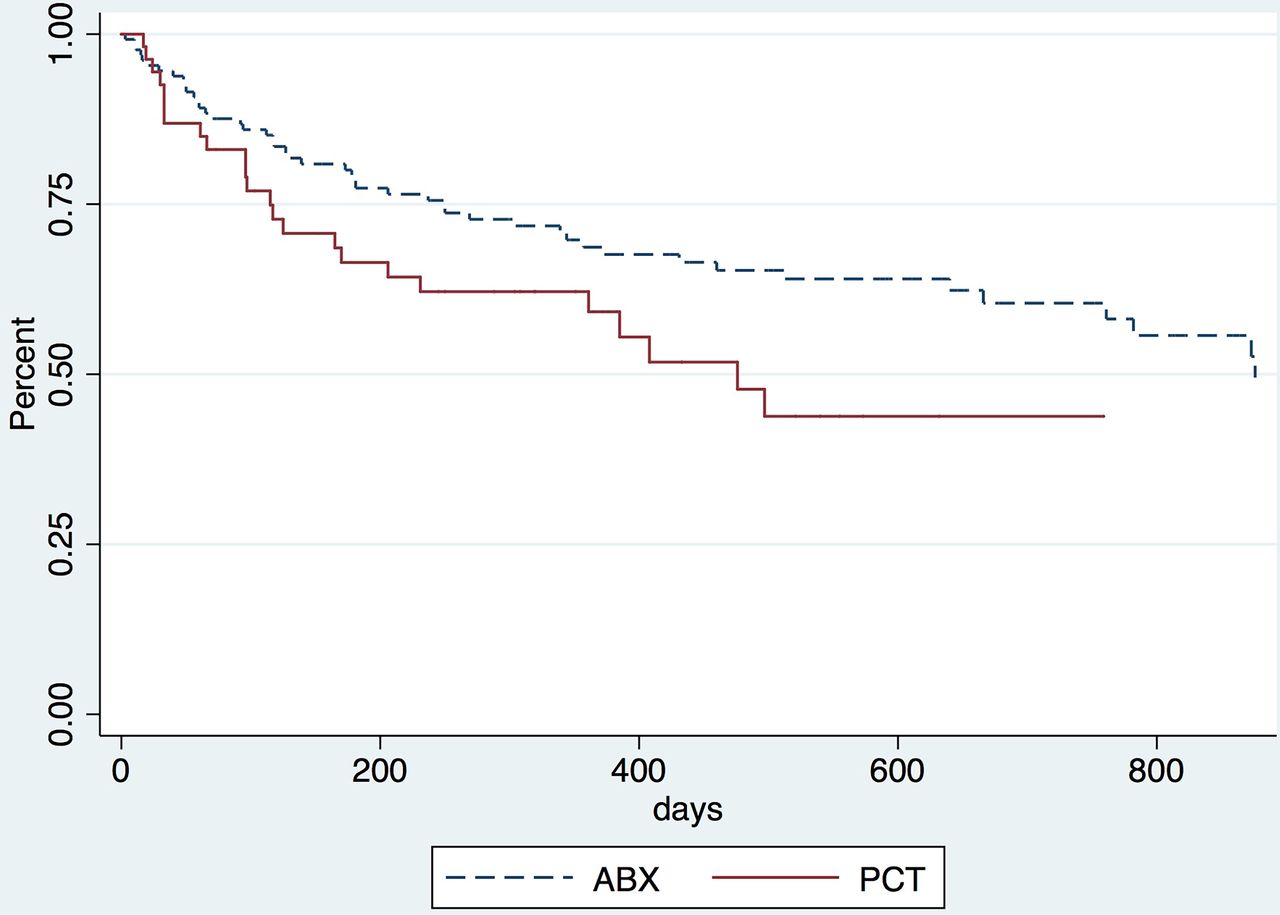
Survival time after initial diagnosis of acute cholecystitis. Log rank p=0.02. ABX, antibiotics; PCT, percutaneous cholecystostomy tube.

Tables
- Table 1
Univariate analysis of factors associated with resolution of acute cholecystitis with ABX versus PCTs
ABX PCT P value Total N 132 54 Age (years), median (IQR) 57 (44–63) 56 (44–66) 0.95 Sex (male) 54 (41%) 27 (28%) 0.87 Stem cell transplant 26 (20%) 8 (15%) 0.30 Hematologic malignancy 52 (39%) 28 (52%) 0.50 Abdominal malignancy 36 (27%) 17 (31%) 1.00 Chemo<6 wks 59 (45%) 31 (57%) 0.61 Abdominal radiation 4 (3.0%) 5 (9.3%) 0.15 Nausea/vmiting 57 (43%) 25 (46%) 0.61 Steroids 18 (14%) 7 (13%) 0.65 ANC (1000 cells/μL), median (IQR) 3.5 (2.2–6.1) 6.0 (1.6–6.2) 0.004 Platelets (1000/mL), median (IQR) 125 (54–199) 153 (63–246) 0.29 Length of stay (days), median (IQR) 5 (2–10) 8 (6–12) 0.02 ASA class I 0 (0%) 0 (0%) 0.04 II 5 (3.8%) 3 (5.6%) III 92 (69.7%) 27 (50%) IV 34 (25.8%) 24 (44%) V 1 (0.8%) 0 (0%) Chemo<6 weeks indicates chemotherapy received less than 6 weeks to presentation.
ABX, antibiotics; ANC, absolute neutrophil count; ASA, American Society of Anesthesiologists; PCT, percutaneous cholecystostomy tube.
- Table 2
Multivariate analysis of factors associated with resolution versus non-resolution of acute cholecystitis
Resolution No resolution N P value OR 95% CI Total N 157 29 186 PCT 51 (94%) 3 (5.6%) 54 0.03 4.89 1.18 to 20.2 Age (years), median (IQR) 57 (44–63) 55 (43–65) 132 0.36 1.02 0.98 to 1.05 Sex (male) 54 (78%) 15 (22%) 69 0.26 0.57 0.21 to 1.52 Abdominal malignancy 36 (92%) 3 (7.7%) 39 0.02 6.66 1.36 to 32.6 Abdominal radiation 4 (57%) 3 (34%) 7 0.01 0.09 0.02 to 0.53 Hematologic malignancy 52 (74%) 18 (26%) 70 0.36 1.83 0.50 to 6.76 Chemo<6 weeks 59 (80%) 15 (20%) 74 0.68 0.81 0.30 to 2.18 Stem cell transplant 26 (20%) 10 (7.6%) 36 0.97 0.98 0.26 to 3.73 ANC (1000 cells/μL), median (IQR) 3.5 (2.2–6.1) 2.6 (1.1–6.2) 125 0.87 0.98 0.90 to 1.06 Steroids 18 (82%) 4 (18%) 22 0.95 0.92 0.07 to 11.3 Length of stay (days), median (IQR) 7 (4–15) 6 (3–10) 186 0.02 0.97 0.94 to 0.99 ASA
III99 (63%) 20 (69%) 119 0.24 0.45 0.12 to 1.69 Chemo<6 weeks indicates chemotherapy received less than 6 weeks to presentation.
Area under the curve=0.78.
ANC, absolute neutrophil count; ASA, American Society of Anesthesiologists; PCT, percutaneous cholecystostomy tube.
- Table 3
Univariate analysis of factors associated IC versus no IC
IC No IC P value Total N 67 90 Age (years), median (IQR) 54 (50–57) 55 (53–58) 0.45 Sex (male) 48 (72%) 33 (37%) 0.63 Stem cell transplant 16 (24%) 18 (20%) 0.56 Hematologic malignancy 32 (48%) 48 (53%) 0.52 Abdominal malignancy 21 (31%) 32 (36%) 0.61 Chemo<6 weeks 33 (49%) 57 (63%) 0.10 Abdominal radiation 2 (3.0%) 7 (7.8%) 0.30 Steroids 8 (12%) 17 (19%) 0.28 Nausea/vomiting 41 (61%) 41 (46%) 0.06 ANC (1000 cells/μL), median (IQR) 6.4 (5.0–7.7) 5.3 (3.8–6.9) 0.36 Platelets (1000/μL), median (IQR) 171 (144–198) 130 (108–152) 0.02 Length of stay (days), median (IQR) 6 (3–9) 6 (3–12) 0.41 ASA I 0 (0%) 0 (0%) 0.58 II 7 (12%) 7 (7.8%) III 48 (80%) 84 (93%) IV 19 (32%) 40 (44%) V 0 (0%) 1 (1.1%) Chemo<6 weeks indicates chemotherapy received less than 6 weeks to presentation.
ANC, absolute neutrophil count; ASA, American Society of Anesthesiologists; IC, interval cholecystectomy; PCT, percutaneous cholecystostomy tube.
- Table 4
Multivariate analysis of factors associated with IC versus no IC
IC No IC N P value OR 95% CI Total N 82 94 176 Age (years), median (IQR) 54 (50–57) 55 (53–58) 176 0.83 1.00 0.97 to 1.02 Sex (male) 48 (72%) 33 (37%) 81 0.62 0.83 0.39 to 1.74 Nausea, vomiting 41 (61%) 41 (46%) 82 0.03 2.30 1.09 to 4.86 Chemo<6 weeksxANC 33 (49%) 57 (63%) 90 0.05 1.14 1.00 to 1.30 Hematologic malignancy 32 (48%) 48 (53%) 80 0.65 1.24 0.49 to 3.15 Steroids 8 (12%) 17 (19%) 25 0.13 0.44 0.15 to 1.27 Platelets (1000/μL), median (IQR) 171 (144–198) 130 (108–152) 173 0.01 1.01 1.00 to 1.01 Stem cell transplant 16 (24%) 18 (20%) 34 0.49 1.46 0.49 to 4.32 Chemo<6 weeks indicates chemotherapy received less than 6 weeks to presentation.
Area under the curve=0.75.
ANC, absolute neutrophil count; IC, interval cholecystectomy; PCT, percutaneous cholecystostomy tube.




{kind=link}
{kind=link}
{kind=link}