

Introduction
This is a recommended evaluation and management algorithm from the Western Trauma Association (WTA) Algorithms Committee addressing the prehospital and in-hospital airway management of adult trauma patients. Because there is a paucity of published prospective randomized clinical trials that have generated class I data, these recommendations are based primarily on published prospective and retrospective cohort studies and expert opinion of the WTA members. The final algorithm is the result of an iterative process including an initial internal review and revision by the WTA Algorithm Committee members and then final revisions based on input during and after presentation of the algorithm to the full WTA membership.
Airway management in the severely injured adult trauma patients begins from the time of first responder arrival and continues until a definitive airway can be established and maintained. Though airway management is important in both the prehospital setting and emergency department, the priorities differ slightly due to alterations in environment, personnel, equipment, expertise and experience. This WTA algorithm will review with most recent evidence and provide recommendations for airway management for the adult trauma patient in both the prehospital setting and emergency department. Cervical spine protection and immobilization, if indicated, will be assumed throughout all airway interventions in the algorithms below. The algorithms (figures 1 and 2) and accompanying comments represent a safe and sensible approach to the evaluation and management of the airway in the acutely injured patient. We recognize that there will be multiple factors that may warrant or require deviation from any single recommended algorithm and that no algorithm can completely replace expert bedside clinical judgment. We encourage institutions to use this as a general framework in the approach to these patients and to customize and adapt the algorithm to better suit the specifics of that program or location.
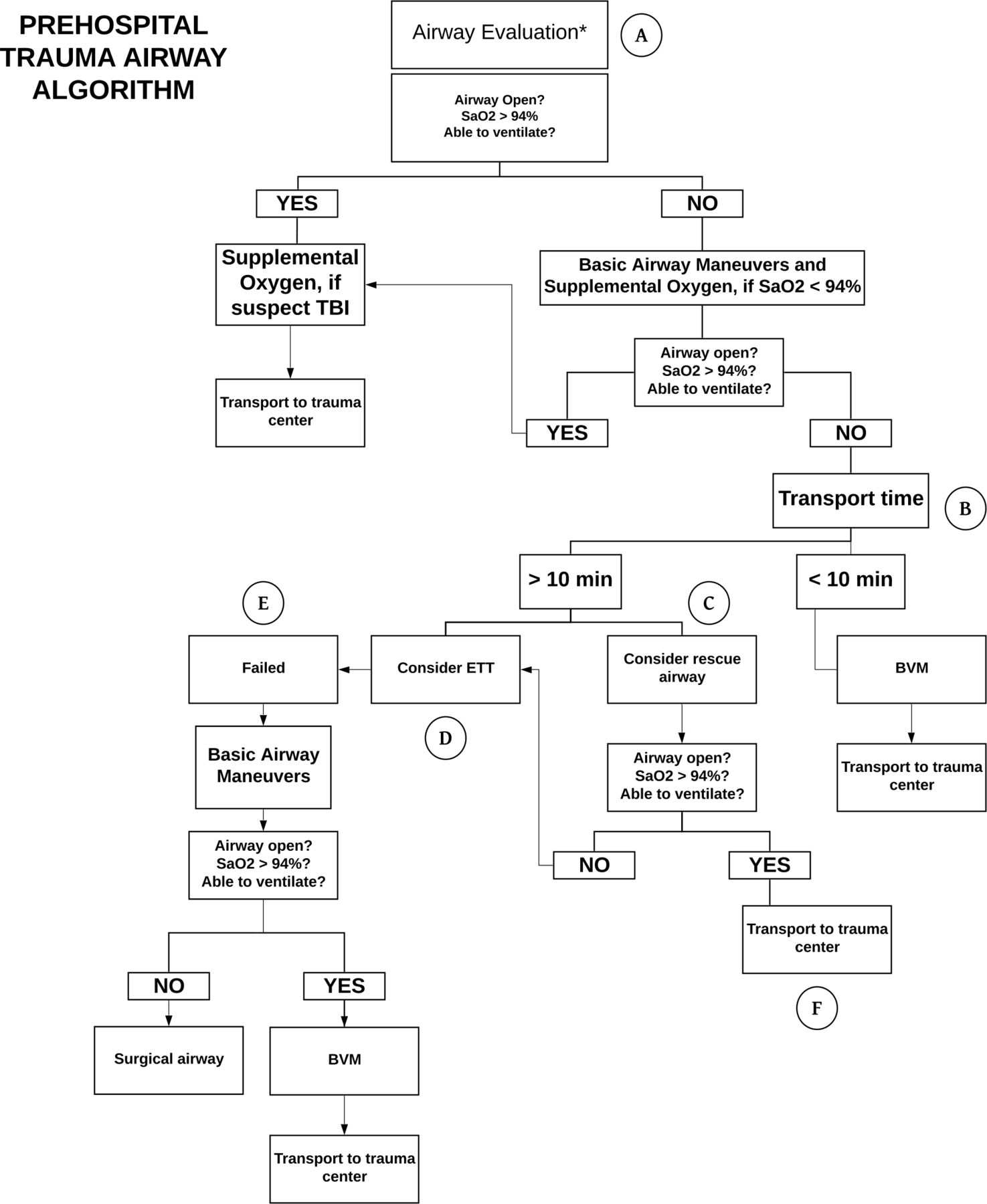
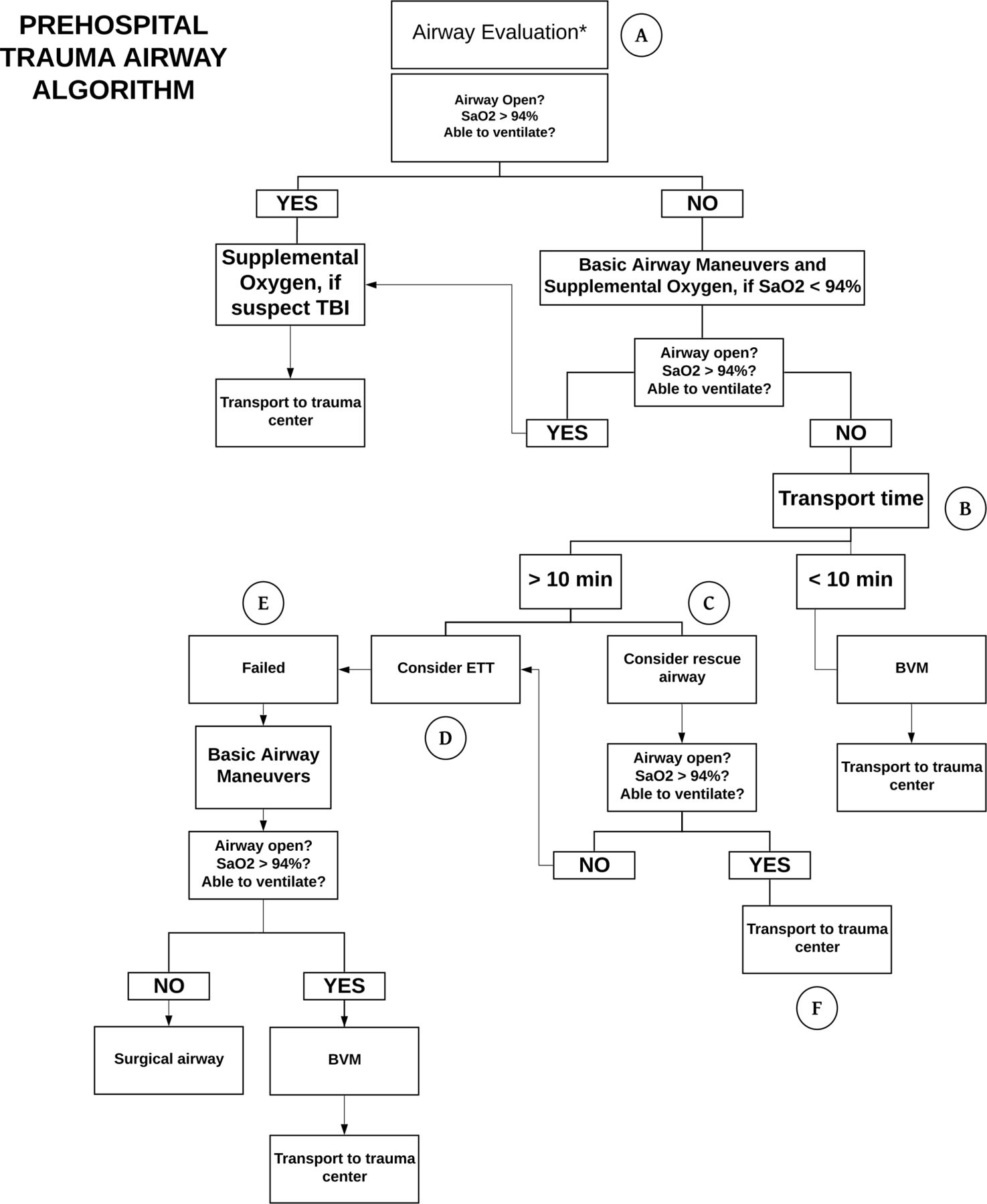
Algorithm for prehospital adult trauma airway management. BVM, bag valve mask.

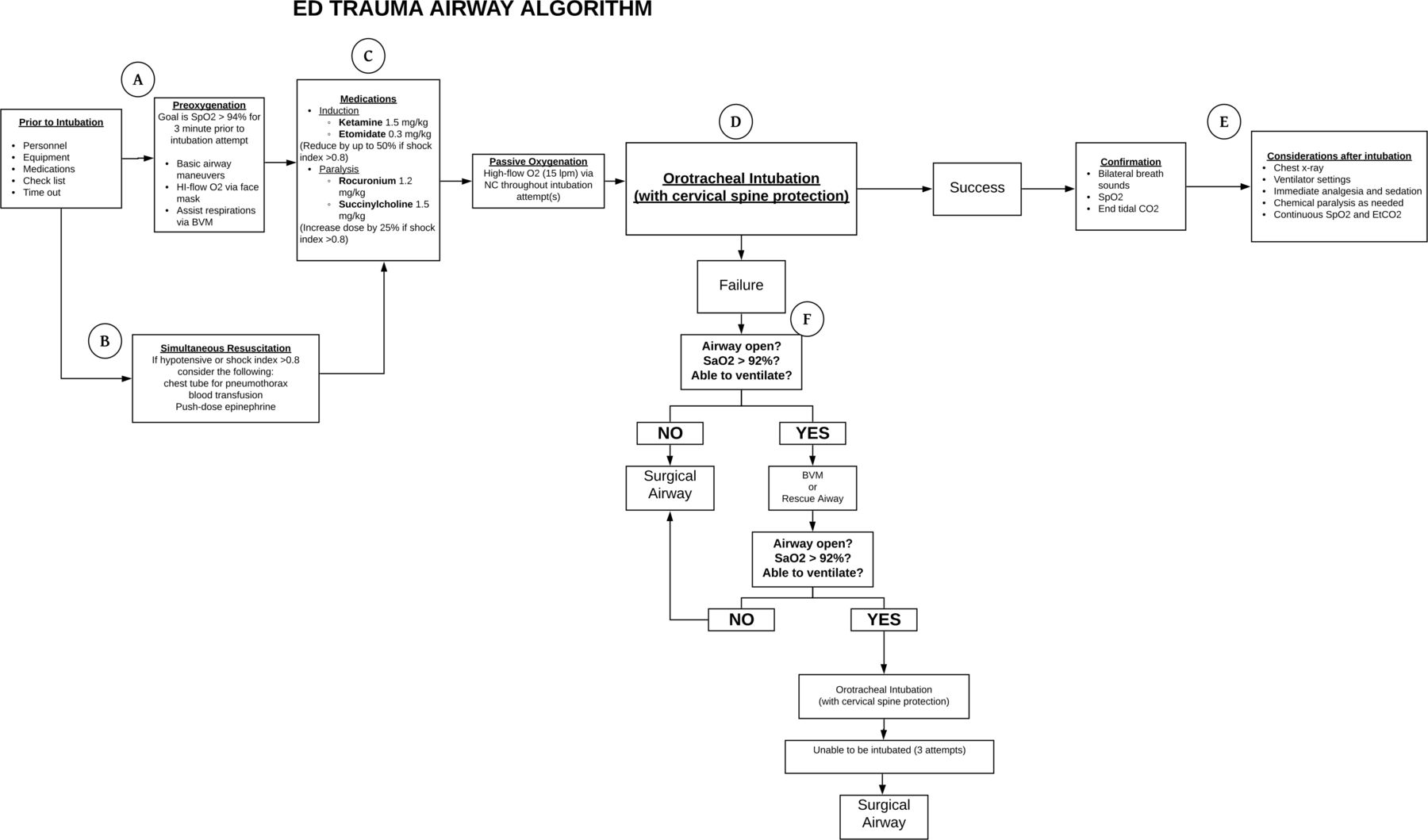
Algorithm for emergency department adult trauma airway management. BVM, bag valve mask; ETT, endotracheal tube; TBI, traumatic brain injury.
Prehospital adult airway management
Airway management is one of the most important components in the prehospital care of the adult trauma patient, as loss of airway may lead to rapid deterioration and death. However, establishing a definitive airway is not always the first priority in the prehospital management of trauma patients. Instead, a focus on an open airway allowing oxygenation and ventilation along with rapid transport to a trauma center should be the main priorities of prehospital trauma airway management. In the vast majority of trauma patients, the airway can be easily management with supplemental oxygen and basic airway maneuvers, deferring placement of a definitive airway to the emergency department.1 2
Prehospital initial evaluation and management
The initial evaluation and management of the prehospital airway should be simplified as much as possible. The first responder should ask a few questions: Is the airway open? Is the oxygen saturation adequate (>94%)? Is the patient ventilating? If the answer to all these questions is “yes,” then the only treatment necessary is supplemental oxygen and the patient can be transferred to the nearest trauma center.3 If the answer to any of these questions is “no,” then the prehospital airway management begins with basic (basic life support) airway maneuvers.4 5 These maneuvers may include a jaw thrust, oropharyngeal airway (OPA), or nasopharyngeal airway (NPA), as long as patient does not have contraindications to OPA (conscious, intact gag reflex) or NPA (basilar skull fracture). After these basic maneuvers, the prehospital provider should ask the same questions: Is the airway open? Is the patient oxygenating? Is the patient ventilating? Once again, if the answer is “yes,” then supplemental oxygen and transport but if the answer is “no,” then next steps in management will depend on transport time to the nearest trauma center.
Prehospital transport time
Transport time is a key variable in management of the prehospital airway. If basic airway maneuvers are not adequate to maintain an open airway, oxygenate, and ventilate, then the patient should be supported with bag-valve-mask (BVM) ventilation. If BVM ventilation is successful (open airway, oxygenating, ventilating) and transport time is short (<10 minutes), then the patient should be transported to the nearest trauma center, providing supplemental oxygen and BVM ventilation.5 If BVM ventilation is not adequate or the transport time is longer (>10 minutes), then consideration should be given to prehospital advanced airway management, this may include rescue airway or orotracheal intubation.
Prehospital rescue airway
The rescue airway (also known as alternative airway, supraglottic airway, or blind insertion airway device) is a relatively new addition to the prehospital armamentarium.6 If BVM ventilation is not effective, then a rescue airway is an excellent next step in prehospital airway management. In addition, BVM is best performed with two providers, one maintaining a mask seal and the other providing manual ventilation. However, in the prehospital setting, a single provider may be required to maintain a seal on the mask as well as provide simultaneous ventilation. If prehospital transport time is long, then solo BVM ventilation may not be practical and a rescue airway may be preferred. These rescue airways may be placed by prehospital personnel and do not require the level of experience or expertise of an orotracheal intubation.7–10
Rescue airway options include Laryngeal Mask Airway, I-gel supraglottic airway, and King LT. The type of rescue airway used is dependent on region of practice and medical direction of the EMS (Emergency Medical Services) agency. Providers must keep in mind that the rescue airway is not a definitive airway, does not prevent aspiration, and may be prone to inappropriate insertion and potential gastric insufflation.
Prehospital orotracheal intubation
In cases where the BVM is inadequate, rescue airways are not available or ineffective, then prehospital orotracheal intubation may be necessary. However, prehospital orotracheal intubation should be reserved for situations with clear indications for definitive airway management and there is experience and expertise available, as prehospital orotracheal intubation has been shown numerous times to be associated with adverse outcomes in trauma patients, particularly in patients with traumatic brain injury.11–17 Causes of worse outcomes of prehospital orotracheal intubation in trauma patients are likely multifactorial and may include lack of experience or expertise, hypoxia, hyperventilation or hypoventilation, misplacement of orotracheal tube, and aspiration. If orotracheal intubation is required, it may be performed in one of three ways, non-medicated intubation, sedation-assisted (without paralytics) intubation, and rapid sequence (sedation and paralysis) intubation. The indications, approach, and medications used for prehospital orotracheal intubation are analyzed by medical direction of the individual EMS agency.
Prehospital failed orotracheal intubation
For a variety of reasons (uncontrolled environment, weather, lighting, operator inexperience, difficult airway) prehospital orotracheal intubation can be challenging and may not be achievable. Multiple attempts at orotracheal intubation should be avoided as these may lead to bleeding and swelling of the airway making subsequent intubation in the emergency department that much more difficult. Instead, in situations where there is failure of orotracheal intubation, the prehospital provider should fall back to basic airway management techniques including jaw thrust, NPA, OPA, BVM, or rescue airway. If all methods fail (cannot intubate, cannot ventilate), which should be a rare occurrence,18 the prehospital provider may be tasked with performing a surgical airway in a trauma patient. Surgical airway options include needle cricothyroidotomy, needle directed percutaneous cricothyroidotomy, or open cricothyroidotomy, with open cricothyroidotomy having higher success rates in the prehospital setting.15–17 However, the indications and technique for a prehospital surgical airway will fall under the medical direction of the individual EMS agency.
Emergency department management of prehospital airway
If a trauma patient arrives to the emergency department with a prehospital airway already in place, several options in management exist. If the patient was orotracheally intubated in the prehospital setting, then the correct position of the tube should be confirmed as discussed later in this manuscript (section below). However, a patient arriving with a prehospital rescue airway in place presents a more complex decision-making scenario. If the patient is not oxygenating or ventilating adequately with the rescue airway, then the patient should be manually ventilated with 100% oxygen to provide as much preoxygenation as possible . While causes of hypoxia/hypoventilation areconcomitantly evaluated, the patient should be orotracheally intubated in a controlled and efficient sequence. However, if the patient is oxygenating and ventilating well with the rescue airway, then the airway exchange to an endotracheal tube can be deferred. It is not clear when that airway exchange should occur, but it should be safe to wait until the primary and secondary survey are complete and exchange the airway in a controlled manner. Regardless of the timing, an exchange of a rescue airway to an endotracheal tube should be assumed to involve a difficult airway as the insertion of rescue devices has been associate with airway injury and edema.19 Another consideration with airway exchange is that some rescue airway devices may be used as a conduit for an airway bougie to facilitate exchange to an orotracheal tube.20
Emergency department adult airway management
Once the adult trauma patient arrives in the emergency department, the environment and options for airway management change significantly. In the emergency department, you have a variety of personnel more experienced in advanced airway management (emergency medicine, respiratory therapy, anesthesia, trauma surgery), a more controlled situation, better lighting, more medication options, and a vast array of equipment including airway adjuncts. However, the guiding principles of airway management remain the same: open airway, oxygenation, and ventilation.
Prior to intubation
The trauma team should make significant preparations prior to patient arrival and planned intubation. Personnel should be gathered prior to patient arrival and for patients with high likelihood for requiring advanced airway management (eg, low GCS (Glasgow Coma Scale)), the entire trauma team should be activated. Every trauma airway should be managed under the premise that there will be a difficult airway, as there is typically not time to complete an evaluation of predictors of difficult laryngoscopy. All advanced airway equipment should be easily accessible and checked for functionality, including laryngoscopes (direct and video), a variety of endotracheal tubes, airway adjuncts (stylets, NPA, and OPAs), rescue airways, and equipment for a surgical airway. Medications needed for rapid sequence intubation should be drawn up and readily available. This preprocedure preparation is an ideal situation for an intubation checklist, or preintubation time out, as these steps have been shown to decrease intubation-related complications and improve adherence to recognized safety measures.21 22
Once the decision has been made to intubate the adult trauma patient, basic airway maneuvers should be used during the time leading up to intubation. Ideally, the patient should have supplemental oxygen applied and preoxygenated for several minutes prior to intubation. Preoxygenation will prolong safe apnea time and prolong apnea time without desaturation.23 If the patient is spontaneously breathing only supplemental oxygen is needed, but if patient is not breathing spontaneously the patient should receive assisted BVM ventilation with jaw thrust, NPA, OPA as needed. Passive oxygenation should continue through the entire intubation process until the definitive airway is secured.
Simultaneous resuscitation
Before and during the intubation process, the severely injured trauma patient should receive simultaneous resuscitation to address abnormalities in breathing and circulation that may be exacerbated during intubation. An existing pneumothorax could be converted to a tension pneumothorax after intubation and positive pressure ventilation, so chest tubes should be considered simultaneous with intubation for patients with an identified pneumothorax. Similarly, intubation and positive pressure ventilation can lead to significant hemodynamic derangement including postintubation hypotension in the apparently stable trauma patient or even cardiac arrest in the trauma patient who arrives hemodynamically unstable.24 25 Postintubation hypotension is associated with increased mortality in trauma patients.26–28 For patients who arrive hemodynamically unstable or stable with a shock index >0.8,29 30 several options for simultaneous resuscitation exist including early blood transfusion using a “circulation first” approach,31 resuscitative endovascular balloon occlusion of the aorta,32 and intravenous push-dose pressors.33 34 In particular, if the airway can be maintained with basic maneuvers and the patient is oxygenating and ventilating, placement of a definitive airway with an endotracheal tube can be deferred until the hemodynamic status of the patient can be addressed.31
Medications
A variety of medications are available to assist with the rapid sequence of adult trauma patients, but the medications can be broken down into two broad categories of induction agents and paralytics. Options for induction agents include sedative/hypnotics (ie, propofol, etomidate, barbiturates, high dose ketamine, high dose benzodiazepines, very high dose opioids), amnestic agents (lower dose benzodiazepines), analgesic agents (ketamine, opioids), with etomidate used most often. Etomidate is dosed at 0.3 mg/kg IV for an induction dose. Etomidate has advantageous characteristics including rapid onset and limited effect on hemodynamics.35 36 The biggest concern with etomidate is adrenal suppression and subsequent decrease in serum cortisol; however, this alteration in lab values has not been associated with adverse clinical outcomes.37 38 Ketamine, dosed at 1.5 mg/kg intravenously, is another option as an induction agent for rapid sequence intubation in trauma patients. It has characteristics that are potentially beneficial in trauma patients including rapid onset, analgesia, amnesia, and sympathomimetic effects and has been shown to have clinical outcomes comparable to etomidate for rapid sequence intubation38–40
Paralytic agents include depolarizing (succinylcholine) and non-depolarizing (rocuronium, pancuronium, vecuronium) agents. Succinylcholine, dosed at 1.5 mg/kg intravenously, is the most common paralytic agent used in trauma intubations. It has a rapid onset and short half-life, making it an ideal agent if there is a failed intubation, allowing quick return of spontaneous respirations. The most common non-depolarizing agent is rocuronium, dosed at 1.2 mg/kg intravenously, and approximates the rapid onset of succinylcholine but has a longer duration of action. Although there are not many direct comparisons of the two drugs, rocuronium has fewer side effects and contraindications and may be associated with lower mortality in patients with severe traumatic brain injury.41 42 As mentioned previously, push-dose pressors may be used to treat or prevent hypotension around the time of intubation.33 34 The two most common agents used are epinephrine and phenylephrine, but epinephrine has the advantage of having both alpha and beta effects. A dilute epinephrine solution may be administered in 5 to 20 μg doses every 2 to 5 minutes to achieve desired effect.
Orotracheal intubation
While preparing for orotracheal intubation, passive oxygenation should continue throughout the intubation process. This can be achieved by placing a nasal cannula on the patien and delivering high-flow oxygen until an endotracheal tube i is placed and confirmed. The placement of the orotracheal tube can be performed via either direct laryngoscopy or video laryngoscopy, and both modalities should be considered complimentary in the management of the difficult trauma airway. Direct laryngoscopy has the advantages of a lower cost, direct view of the airway (three dimensional, maintain depth perception) and is less prone to have view obscured due to fog or blood on video camera.43 However, video laryngoscopy has made a significant impact in airway management and may now be the preferred technique for trauma intubations. Video laryngoscopy offers numerous advantages over direct laryngoscopy including: superior views of the glottis (Cormack-Lehane I/II), higher intubation success rates for patients with anatomically difficult airways, in obese patients, and in those with the cervical spine held in-line, less spine movement, and higher intubation success rates by inexperienced airway providers.44 45 In addition, a recent Cochrane Review concluded that video laryngoscopy improves glottic views, decreases airway trauma, and reduces the number of failed intubations, particularly in patients with a difficult airway.45
Confirmation of orotracheal tube placement
Once the patient has been orotracheally intubated, the next priority is confirmation of endotracheal tube position. The tube should be inserted to about 21 cm for women and 23 cm for men, when measuring from the corner of the mouth. There are several indicators of appropriate tube placement including tube condensation, chest rise and fall, and breath sounds, but the most accurate confirmatory tests for tube confirmation are seeing the tube go through the cords at intubation and end tidal CO2 measurement.46 This can initially be performed with a colorimetric CO2 monitor that changes color when it contacts the expired CO2 but can then be switched to a capnographer that can display an end tidal CO2 value and a graphical tracing on the monitor. Once the tube is confirmed with CO2, it can be secured and a chest X-ray performed to evaluate the depth of tube insertion and appropriate position 2 to 3 cm above the carina.47 Depending on which medications were used for induction and paralysis, consideration should be given for providing the patient with longer acting pain medicine, sedation, and potentially paralysis for the subsequent trauma evaluation and treatment. In the event of postintubation hypotension, the physician should confirm appropriate ventilator settings, evaluate for tension pneumothorax, and look for sources of ongoing hemorrhage.
Failed orotracheal intubation
Several difficult airway algorithms exist that offer options in the situation if failed orotracheal intubation, including the commonly cited algorithm from the American Society of Anesthesia.48 However, many of the options available in the management of the elective airway (awake fiberoptic intubation, awakening the patient) are not applicable in the trauma airway management. For a trauma patient, if initial orotracheal intubation fails, the first step is to revert back to basic airway maneuvers and analyze if the airway can be supported with noninvasive methods. The patient should receive a jaw thrust, an OPA, supplemental oxygen, and receive BVM ventilation and then ask the questions: Is the airway open? Is the patient oxygenating? Is the patient ventilating? If the answer to these questions is “no,” then the patient should receive a surgical airway. If the answer to these questions is “yes,” then the patient can be supported, and a clear plan can be developed for the next attempt at orotracheal intubation. While oxygenating and ventilating the patient noninvasively, several things should be considered prior to the next attempt.
If not already done so, additional equipment should be gathered including smaller endotracheal tubes, bougies (gum elastic, lighted), direct laryngoscope if videolaryngoscopy was initially used and vice versa, alternative blades (Miller versus Macintosh) for the direct laryngoscope, rescue airways, and the surgical airway instrument tray should be opened. The view of the airway (blood, edema, Cormack-Lehane view) should be discussed to analyze the difficulty of the next attempt. Depending who performed the first attempt, the next attempt should be performed by a more experienced operator, likely the most experienced in the room.49 If anesthesia has not already responded to the trauma activation, they should be summoned to the room to increase the number of team members with advanced airway experience and expertise. Prior to the next attempt, the patient should once again receive preoxygenation as this will allow safe apnea time for the next attempt, which will presumably be more difficult and may take longer. This is an important step, if possible, as the time it takes for oxygen saturation to drop from 90% to 60% is much faster than the time it takes to drop from 100% to 90%.50 The closer the oxygen saturation can get to 100%, the more time the team will have for the next attempt. Once the situation is optimized a second intubation can be attempted (or at most three attempts), if this fails the patient should receive a surgical airway.
Areas of controversy and existing knowledge/research gaps
During preparation of this algorithm and manuscript, there were areas of controversy among the committee that deserve further mention. Much of the disagreement surrounded the number of intubation attempts that should be performed. The number of attempts performed depends on several factors including the experience of the intubating provider, the physiologic status of the patient, and the presence of modifiable factors during the attempt at intubation. Though the algorithm states that a surgical airway should be performed after three failed attempts, there are clearly situations where a surgical airway would be performed before three attempts. If the first attempt is performed by an experienced operator and the airway is analyzed to edematous or distorted (from direct trauma, prehospital intubation attempts, or prior rescue airway placement), then a surgical airway should be considered after the failed first attempt, rather than further trials of orotracheal intubation. There was also some variability in the prehospital transport time limit that would differentiate a “rapid” transport from a “prolonged” transport time where intubation should be more heavily favored. We achieved consensus on a time of 10 minutes, but this should not be taken as an exact cutoff and this time should be individualized to each EMS system.
It is also important to note that there are many areas of this algorithm that lack high quality evidentiary support, and where further focused research is required. Table 1 provides a list of the most important specific topics or existing research “gaps” related to this topic that were identified by the authors during the development of this algorithm.
Top identified knowledge and research gaps related to trauma airway management
Conclusion
Airway management is an obvious priority throughout the spectrum of care for an adult trauma patient. Rather than a definitive airway, the goal of prehospital adult airway management is to obtain an open airway to oxygenate and ventilate the patient. This can generally be achieved with noninvasive methods of jaw thrust, NPA, OPA, supplemental oxygen, and BVM ventilation. In fact, these noninvasive methods are the most important components of advanced airway management of the adult trauma patient in both the prehospital setting and the emergency department. Once in the emergency department, the adult trauma patient with a compromised airway will require definitive management, and in the adult trauma patient, this is most often achieved through orotracheal intubation. This procedure requires detailed planning and preparation and an organized approach for success. We hope this article provides the practitioner a concise review and recommended algorithm for airway management in the adult trauma patient.
Footnotes
Presented at This was an oral presentation at the 49th Annual Meeting of the Western Trauma Association, March 3–8, 2019, Snowmass, Colorado.
Contributors All authors meet authorship criteria for this manuscript as described below. All authors have seen and approved the final manuscript as submitted. The first author (CVRB) had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Literature review: CVRB. Study design: CVRB, KI, DVS, EEM, DC, JAS, HBA, KB, MM, JLS, AGR. Data interpretation: CVRB, KI, DVS, EEM, DC, JAS, HBA, KB, MM. Writing: CVRB. Critical revision: CVRB, KI, DVS, EEM, DC, JAS, HBA, KB, MM, JLS, AGR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}