

Abstract
Background Although helmets are associated with reduction in mortality from motorcycle collisions, many states have failed to adopt universal helmet laws for motorcyclists, in part on the grounds that prior research is limited by study design (historical controls) and confounding variables. The goal of this study was to evaluate the association of helmet use in motorcycle collisions with hospital charges and mortality in trauma patients with propensity score analysis in a state without a universal helmet law.
Methods Motorcycle collision data from the Arizona State Trauma Registry from 2014 to 2017 were propensity score matched by regressing helmet use on patient age, sex, race/ethnicity, alcohol intoxication, illicit drug use, and comorbidities. Linear and logistic regression models were used to evaluate the impact of helmet use.
Results Our sample consisted of 6849 cases, of which 3699 (54.0%) were helmeted and 3150 (46.0%) without helmets. The cohort was 88.1% male with an average age of 40.9±16.0 years. Helmeted patients were less likely to be admitted to the intensive care unit (20.3% vs. 23.7%, OR 0.82 (0.72–0.93)) and ventilated (7.8% vs. 12.0%, OR 0.62 (0.52–0.75)). Propensity-matched analyses consisted of 2541 pairs and demonstrated helmet use to be associated with an 8% decrease in hospital charges (B −0.075 (0.034)) and a 56% decrease in mortality (OR 0.44 (0.31–0.58)).
Discussion In a state without mandated helmet use for all motorcyclists, the burden of the unhelmeted rider is significant with respect to lives lost and healthcare charges incurred. Although the helmet law debate with respect to civil liberties is complex and unsettled, it appears clear that helmet use is strongly associated with both survival and less economic encumbrance on the state.
Level of evidence Level III, prognostic and epidemiological.
Introduction
More than 70% of non-helmeted motorcycle crash (MCC) patients die at the scene of the collision, and the remaining 30% that are hospitalized have a higher Injury Severity Score, are more likely to require intensive care unit (ICU) treatment and mechanical ventilation, and are more likely to die in hospital when compared with helmeted motorcyclists.1–4 This increased morbidity and mortality leads to a difference of $2.2 billion spent on non-helmeted motorcyclists in terms of production lost.5 Since the 1990s, annual motorcycle deaths have more than doubled gradually rising from a low of 2116 in 1997 to their peak of 5337 in 2016.6
Nonetheless, the right of a motorcyclist to choose not to wear a helmet remains a contentious issue in the USA. In addition to arguments specific to civil liberty, opponents of helmet laws contend that the extant research supporting the benefit of helmets is compromised by study design (namely the use of historical controls) and significant confounding of age, socioeconomic status, race, health insurance status, and alcohol/illicit drug use.
To overcome the limitations of previous studies, we performed a comparative analysis of helmeted versus non-helmeted motorcyclists in the state of Arizona, where only motorcyclists under the age of 18 are required by law to wear a helmet. Specifically, using the Arizona Trauma Registry maintained by the Arizona Department of Health and Safety, the association between helmet use and both mortality and hospital charges, with adjustment for relevant confounding variables, was evaluated by propensity score analysis. We hypothesized that helmet use would be associated with decreased mortality and hospital charges.
Patients and methods
The Arizona Trauma Registry is maintained by the Arizona Department of Health Services. The registry’s purpose is to track patient demographics, injury patterns, complications, and mortality at all trauma centers in Arizona. All state-designated trauma centers in Arizona are mandated to submit data at the patient level to the state-wide registry on a quarterly basis. Records involving a motorcycle collision with the motorcycle driver or passenger patient admitted to a state-designated level 1 trauma center in Arizona between January 1, 2014 and December 31, 2017 were queried. Data points included: patient demographics and injury characteristics, helmet use, discharge status, hospital length of stay, ICU length of stay, mortality and total hospital charges.
Statistical analysis
Hospital charges were inflated to 2017 dollars using the Consumer Price Index by adjusting hospital charges for each case by adding the following percentage for each year: 2014 (3%), 2015 (3%), 2016 (2%).7 After an assessment for normality, hospital charges and length of stay were natural log transformed. Matching was used to minimize significant differences in patient demographics between the groups of patients wearing or not wearing a helmet. A propensity score for each case was created by regressing helmet use on age, sex, race/ethnicity, alcohol above legal limit at time of collision, illicit drug use at time of collision, patient comorbidities, and payer source (insurance status of the patient). A 1:1 match was then done using the Greedy algorithm on propensity score with the Mahalanobis distance calculation method and a force match on sex, race/ethnicity, alcohol and illicit drugs.
Cohort characteristics between patients wearing versus not wearing a helmet were compared using paired samples t-tests and Mantel-Haenszel χ2 tests accounting for each matched pair. Linear and logistic multivariate regression models were used to evaluate the impact of helmet use and other covariates on hospital charges and mortality. Covariates in these models included patient age, sex, alcohol above the legal limit, the number of patient comorbidities, toxicology results of illicit drugs, race/ethnicity, and payer source. NCSS V.10 was used for matching and SPSS V.25 was used for all other analyses.
Results
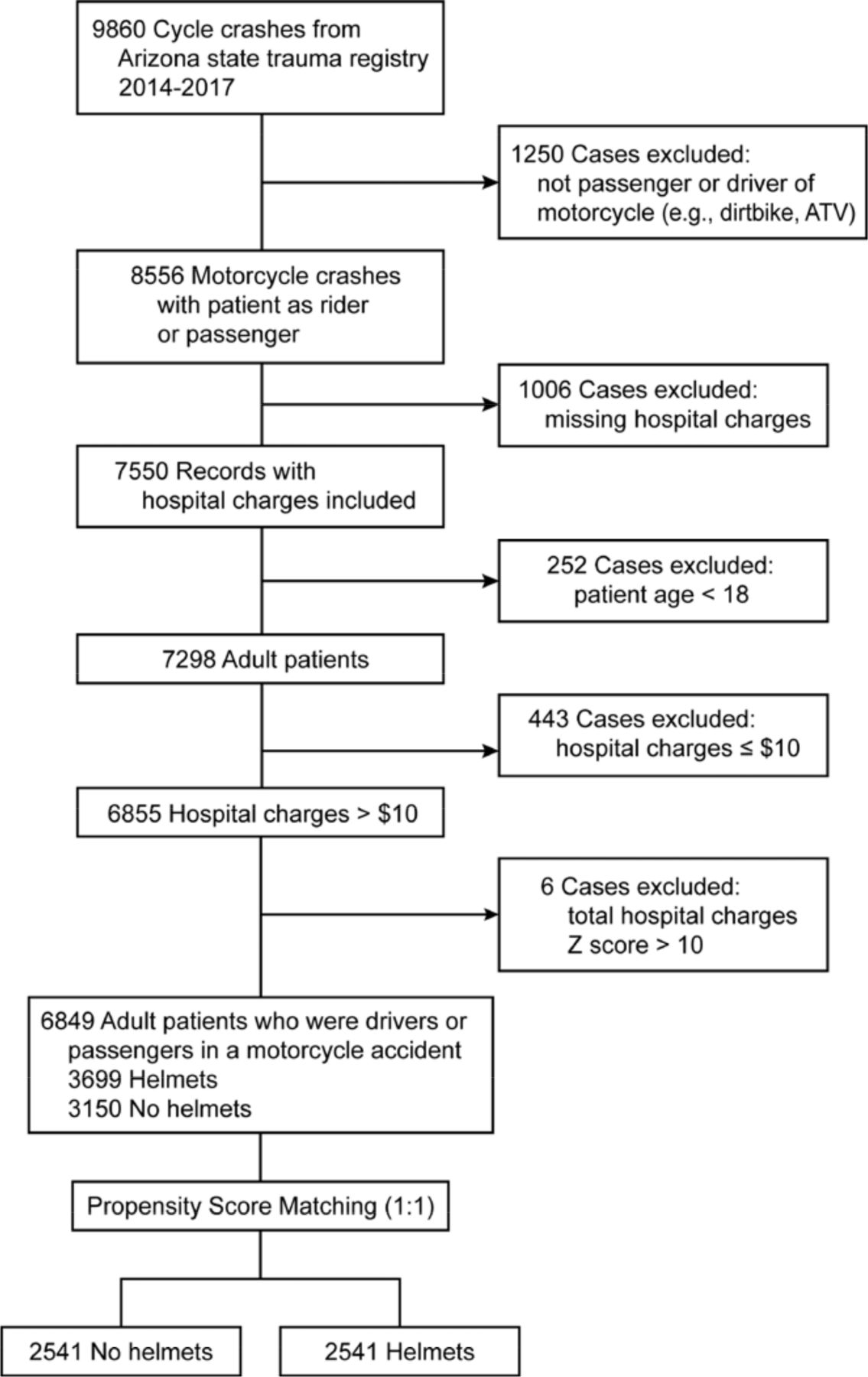
The state trauma registry provided 9860 patient records during the period of study. Cases were excluded if the patient was not a driver or passenger on a motorcycle, if less than 18 years of age, had a file with missing data, or was determined to be an outlier based on hospital charges (figure 1). Our sample consisted of 6849 cases, of which 3699 (54.0%) were helmeted and 3150 (46.0%) without helmets. There were significant differences between the two groups regarding average age, the proportion of cases with one or more comorbidities, toxicology results of alcohol above the legal limit (0.08) and illicit drug use (table 1).
Summary of patient demographics and toxicology screen prior to matching

Patient flow diagram. ATV, all-terrain vehicle.
The distribution of race and payer mix also varied significantly between groups. To account for these differences propensity score matching was used. Our propensity match yielded 2541 pairs and the standardized difference for the propensity score decreased to 1.44% for the matched sample, well under the 10% standard. The matched results are shown in table 2 with a perfect match reflected for all categorical variables (p=1.000). Mean age continued to be significant with an average age of 42.5±15.5 years for no helmet versus 39.2±16.4 years for helmeted patients; however, with a Cohen’s d effect size decreasing from 0.3 in the unmatched sample to 0.2 in the matched sample reflecting a smaller difference between the means and a smaller effect size.
Summary of matched variables in the matched cohort
In the matched sample, differences remained between the helmet and no helmet groups for injury severity (6.0 vs. 5.0; p=0.013), Glasgow Coma Scale score less than 15 (17.0% vs. 10.0%; p<0.001), the proportion of patients ventilated (12.0% vs. 7.8%; p<0.001), admitted to the ICU (23.7% vs. 20.3%; p=0.002), and mortality (5.4% vs. 2.4%; p<0.001) with the no helmet group associated with patient gravity (table 3).
Summary of injury severity, length of stay and patient outcomes between groups
A summary of adjusted multivariate linear regression models predicting hospital charges is shown in table 4. In the matched sample, helmet use was a significant and negative predictor of charges (p=0.029) with helmet use associated with an average decrease in hospital charges of 8%. This same model was calculated on the entire sample, the results are nearly the same with helmet use also associated with an average decrease in hospital charges of 8% (p=0.009).
Summary of linear regression predicting total hospital charges (ln)
Adjusted multivariate logistic models predicting mortality are summarized in table 5. Helmet use emerged as a negative predictor of death in both the matched model (p<0.001) and the model based on the entire sample (p<0.001). Interpretation based on the OR suggested for each death, a 56% decrease in the odds of wearing a helmet in the matched sample and a 54% decrease in the model based on the entire sample.
Summary of logistic regression predicting mortality
Discussion
In our study we used propensity score matching to attempt to create two balanced groups and control for known confounding variables, and think we are the first to apply this type of analytic strategy to evaluating the impact of helmet use on outcomes and hospital charges among patients injured exclusively on motorcycles. Our findings are in line with the findings based on unmatched analyses and suggest helmet use is associated with superior patient outcomes and decreased hospital charges.
Motorcycle collisions have been on the rise during the last two decades in Arizona with 150 fatalities reported in 2018 compared with 60 in 1997.8 Our analysis recapitulated the benefits of helmet use by demonstrating that non-helmeted riders suffered a higher severity of injury, were more likely to be admitted to the ICU and require mechanical ventilation, and die during their hospital admission. These results are intuitive considering the known safety benefits of wearing a helmet. After passing mandatory helmet laws, the states often see a sharp decline in fatalities and head injuries. Neighboring California saw a 37.5% decrease in fatalities after mandating helmet use in 1992.9 Nebraska saw similar declines in the rate of motorcycle collisions (26%) along with fewer serious head injuries, hospital admissions, and deaths from 1989 to 1990 after passing universal helmet use in 1989.10
Less severely injured patients translated into healthcare savings. We performed a linear regression of our matched patients to see how much motorcycle helmets saved hospitals and found there was an 8% reduction in overall healthcare charges associated with wearing a helmet. Similar results were found by Philip et al in 2013 where non-helmeted patients accrued an average of $20 065 more in hospital cost after adjusting for age, sex, and insurance payer.11 Eastridge et al estimated that from 1994 to 2002 non-helmeted MCC patients requiring transport to a hospital admission required care costing $250 231 734 more per year than helmeted patients.12 If there were mandated helmet laws for every state, Dua et al2 in 2015 estimated the national savings to be $2.2 billion per year.
The present study is notable for several strengths and limitations. Strengths include the utilization of matching by propensity scoring in the study design. This analysis allows for adjustment for confounding variables including insurance status and contribution of alcohol and/or illicit drug use to injury; prior studies have been criticized for failure to account for these important potentially confounding variables. In addition, many of the prior studies that demonstrate a benefit to helmet use are constructed to compare outcomes before and after enactment of helmet laws. Such study designs that rely on historical controls are prone to the influence of underlying confounders related to differences related to the time periods of study. The matched cohort design of the current study avoids the issue of temporal inconsistency. Lastly, the use of a state-wide registry provides a relatively useful statistical picture of helmet use in the state of Arizona that is relatively more robust than reports from single institutions or selected multi-institutional studies.
Limitations of the study include the potential for selection bias. The study base was derived from patients transported to level 1 trauma centers and thus the outcomes of patients who either died at the scene of injury or were not transported to a trauma center are not included in our analysis. In addition, granular details regarding the type of helmet worn, whether the helmet was worn properly, and the influence of ambient light, weather, and the precise nature of the collision are not contained in the state’s registry, and might influence the results of our analysis. Although the comparative groups in this study were adjusted for known confounders such as insurance status, it is possible that unknown confounders may be present and influence our results. Lastly, data specific to differences or similarities in injury types and anatomic locations sustained between groups, as well as cause of death, were not available to the researchers and would certainly inform the discussion surrounding helmet use.
In summary, we have observed that in a state without mandated helmet use for all motorcyclists, the burden of the non-helmeted rider is significant with respect to lives lost and healthcare charges incurred. These findings are not novel. Nonetheless, we think the strengths of our study, including its size and methodology, strengthen the argument to mandate helmet use for motorcycle riders. Although the helmet law debate with respect to civil liberties is complex and unsettled, it appears clear that helmet use in Arizona is strongly associated with survival and decreased hospital charges.
Footnotes
Contributors MDJ participated in the study design, article preparation, and interpretation. JGE and DV participated in the study design and interpretation. KMC participated in the data collection, analysis, and article preparation. JNB participated in the study design, interpretation, and critical review. JAW participated in the study design, interpretation, article preparation, and critical review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study obtained approval from the St Joseph’s Hospital and Medical Center’s internal Institutional Review Board (IRB; approval number: PHXA-18-500-230-73-21) and the Arizona Department of Health Services IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}