

Article Figures & Data
Figures
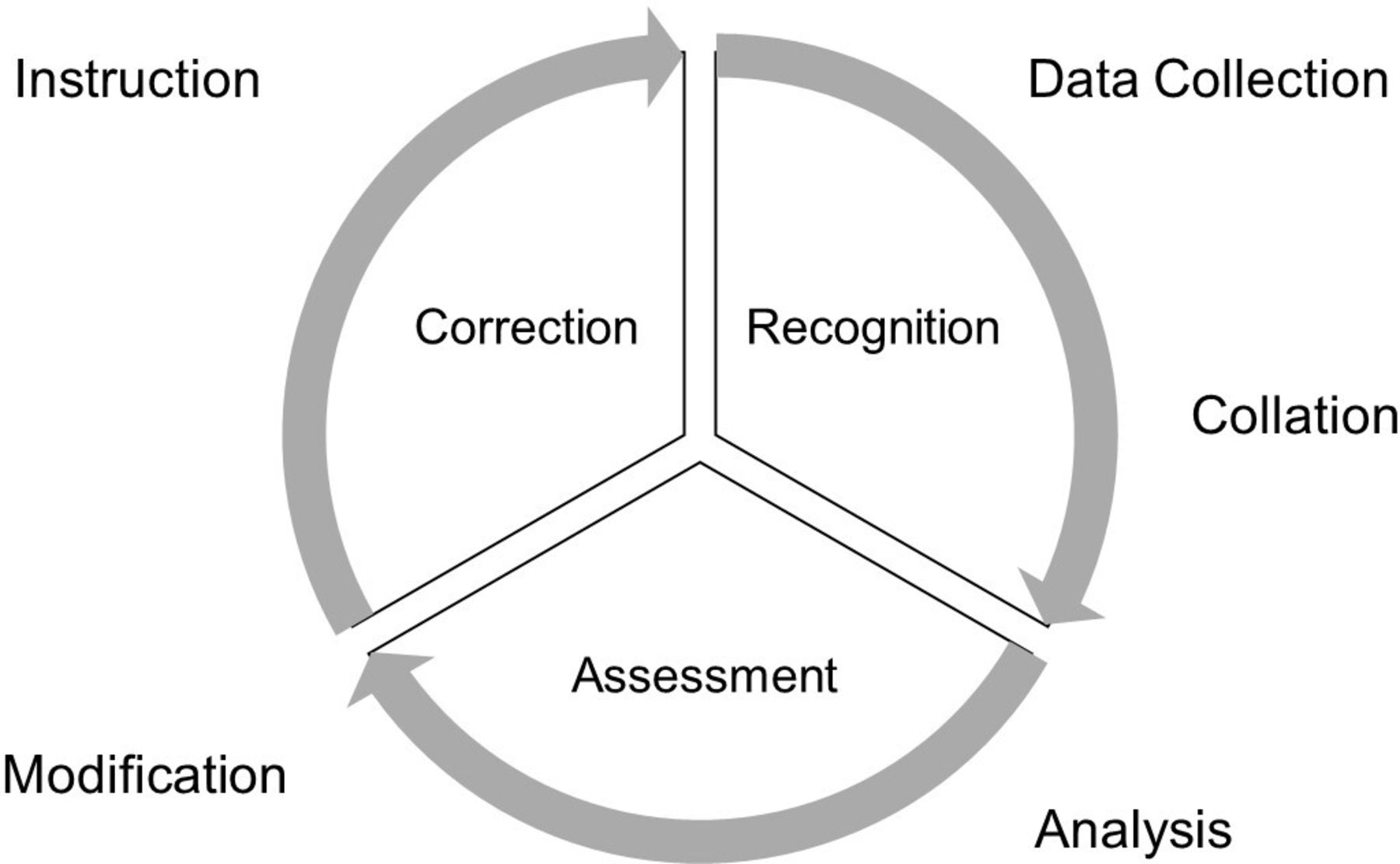
- Figure 1
Continuous process of performance improvement.
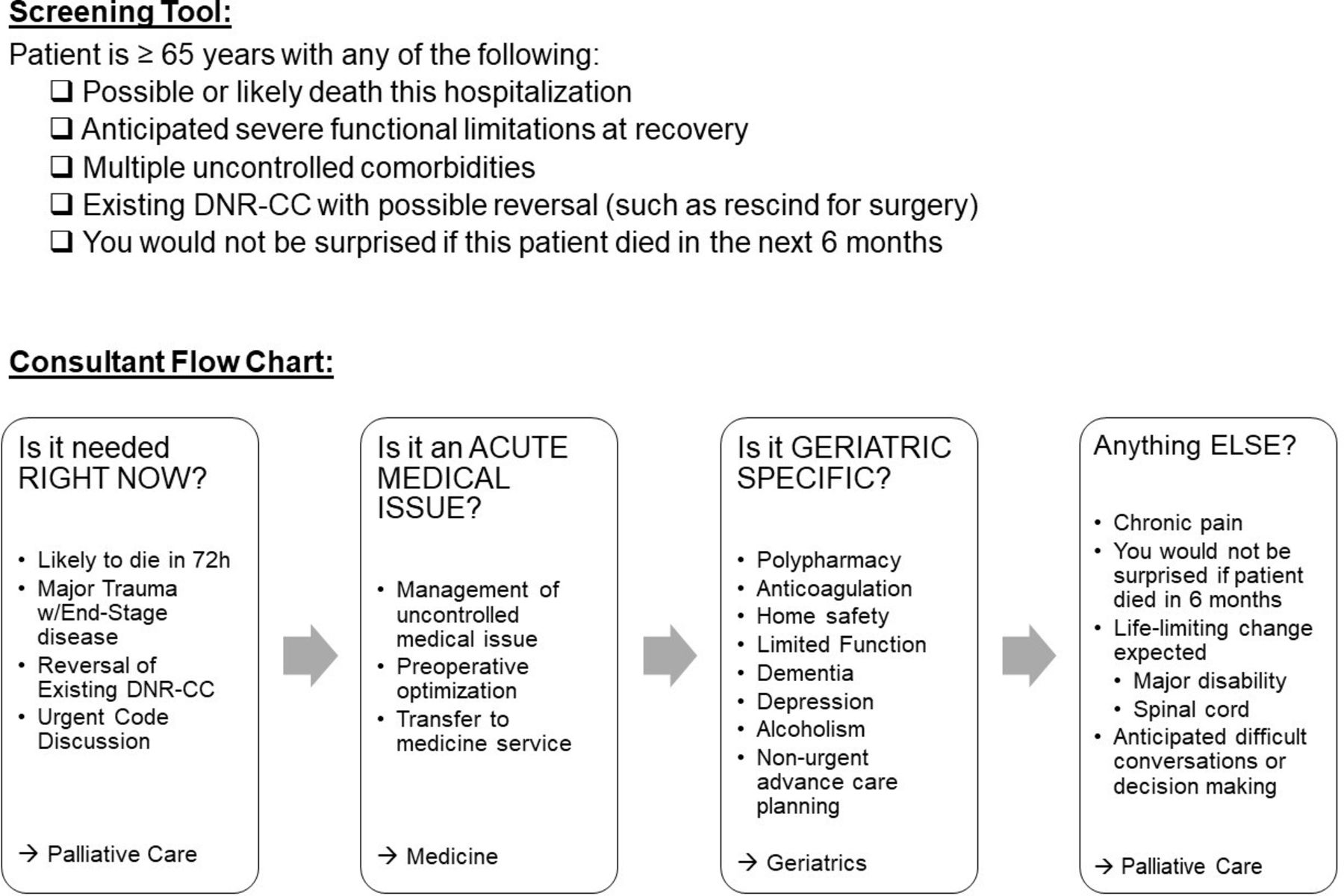
- Figure 2
Trigger tool and flowchart of consultations. DNR-CC: Do Not Resuscitate-Comfort Care
Tables
- Table 1
Examples of palliative care gap analysis*
Palliative care guideline Met Partially met Unmet Status Comments Screen/identify early at-risk ED patients. Communicate difficult news after sudden traumatic death. Early goals of care conversations. Obtain advance directives and Medical Orders for Life-Sustaining Treatment (MOLST)/Physician Orders for Life-Sustaining Treatment (POLST) forms. Family presence in resuscitation. Assess all seriously ill patients for palliative care needs. Palliative care is delivered in conjunction with curative, life-prolonging or disease-modifying trauma care. Palliative care is delivered by an interdisciplinary team. Pain and symptom management, communication, and prognostication are provided. Patients and families receive education about their condition, its impact on prognosis, and healthcare trajectory. A predictive or prognostic tool is used for estimating survival time and tracking palliative care needs. Identification of the surrogate or proxy decision maker is documented on patient’s medical record within 24 hours of admission. The advance care plan is discussed and developed with patient/family within 72 hours. Family meetings are used early to discuss outcomes, expectations and goals of care. Psychosocial/emotional support is assessed and a plan is created. *Adapted from the American College of Surgeons Trauma Quality Improvement Project Palliative Care Best Practices Guidelines (https://www.facs.org/-/media/files/quality-programs/trauma/tqip/palliative_guidelines.ashx, accessed October 5, 2020).
- Table 2
Examples of geriatric care gap analysis
Geriatric trauma management guideline Met Partially met Unmet Priority Comments Trauma registry criteria include same height falls. Geriatric trauma management activation protocol is documented. Geriatric specific resuscitation guidelines are documented. Geriatric guidelines address the changes in the Glasgow Coma Scale (GCS), and dementia assessment is documented. Specific lab values for geriatric trauma resuscitations are documented. Pain management guidelines for geriatric trauma patients are documented. Specific precautions to prevent hypothermia and skin injury are documented. Time frames for frailty assessment are documented. Capacity assessment guidelines are documented. Goals of care are documented in the phases of care. Prognostic tools are available to assist in documentation. Guidelines include assessment, interventions, and reversal agents for anticoagulation management, as well as restarting therapy after operative interventions. Medical management and reconciliation guidelines define when and how often this is completed and documented. Beers criteria are included in the medication management Guideline includes geriatric trauma intensive care unit admission criteria and is documented. *Adapted from the updated American College of Surgeons Trauma Quality Improvement Project Geriatric Trauma Management Best Practice Guideline, currently submitted for publication.




{kind=link}
{kind=link}
- Article
- Abstract
- Introduction
- Verification, review, and consultation perspective
- Implementation strategy: education perspective from University of Texas Health Science Center at Houston (UT Houston)
- Strategy: consultation tool perspective from MetroHealth Medical Center
- Implementation strategy: frailty screen: perspective from Harborview Medical Center (HMC)
- Conclusions
- Data availability statement
- Ethics statements
- Footnotes
- References
- Figures & Data
- eLetters
- Info & Metrics