

Abstract
Objectives Comparisons of risk-adjusted trauma mortality between high-income countries and low and middle-income countries (LMICs) can be used to identify specific patient populations and injury patterns for targeted interventions. Due to a paucity of granular patient and injury data from LMICs, there is a lack of such comparisons. This study aims to identify independent predictors of trauma mortality and significant differences between India and the USA.
Methods A retrospective cohort study of two trauma databases was conducted. Demographic, injury, physiologic, anatomic and outcome data were analyzed from India’s Towards Improved Trauma Care Outcomes project database and the US National Trauma Data Bank from 2013 to 2015. Multivariate logistic regression analyses were performed to determine significant independent predictors of mortality.
Results 687 407 adult trauma patients were included (India 11 796; USA 675 611). Patients from India were significantly younger with greater male preponderance, a higher proportion presented with physiologic abnormalities and suffered higher mortality rates (23.2% vs. 2.8%). When controlling for age, sex, physiologic abnormalities, and injury severity, sustaining an injury in India was the strongest predictor of mortality (OR 13.85, 95% CI 13.05 to 14.69). On subgroup analyses, the greatest mortality difference was seen in patients with lower Injury Severity Scores.
Conclusion After adjusting for demographic, physiologic abnormalities, and injury severity, trauma-related mortality was found to be significantly higher in India. When compared with trauma patients in the USA, the odds of mortality are most notably different among patients with lower Injury Severity Scores. While troubling, this suggests that relatively simple, low-cost interventions focused on standard timely trauma care, early imaging, and protocolized treatment pathways could result in substantial improvements for injury mortality in India, and potentially other LMICs.
Level of evidence Level 3, retrospective cohort study.
Introduction
Trauma is a leading cause of death globally, claiming more than 5 million lives, and nearly 1 billion people require medical care for injuries annually.1 2 For perspective, the global burden of injury accounts for 32% more fatalities than malaria, tuberculosis and HIV/AIDS combined.2 Additionally, among those aged 5–45, trauma is the leading cause of disability-adjusted life-years.3 Premature deaths and prolonged disability due to injury inflict a substantial economic toll.4 5 Road traffic injuries alone, which account for less than a third of injuries globally, have been estimated to cost up to 2% of a country’s gross national product.5
Nearly 90% of injury-related deaths occur in low and middle-income countries (LMICs), and if fatality rates among the injured in LMICs were similar to those in high-income countries (HICs), nearly 2 million lives could be saved annually.5 6 Over 20% of the world’s trauma deaths occur in India,7 where injuries have been identified as a major public health problem.8–11 Furthermore, in a Delphi study of injury-related deaths in India, over half of the deaths were deemed preventable.12
Trauma research and monitoring is an essential component of advanced trauma systems that have evolved in HICs.13–16 Despite the substantial burden of injury in LMICs, most trauma care research is conducted in HICs.17 18 Lack of injury information and research remains a challenge in LMICs, and has been identified as a major barrier to global emergency and trauma care system development.17–19 To address this gap, the Towards Improved Trauma Care Outcomes (TITCO) data project was developed to improve trauma care information systems in India and systematically collect essential injury data.20
Comparisons of risk-adjusted trauma mortality between HICs and LMICs can be used to identify specific patient populations and injury patterns for targeted interventions. Due to a paucity of granular patient and injury data from LMICs, there is a lack of such comparisons. The current study aims at addressing this gap in knowledge by identifying independent predictors of trauma mortality with a detailed analysis of differences in demographics, physiology, injury burden, and injury mortality between India and the USA. Such an analysis could allow for identification of specific gaps in care and potential targets for reduction in trauma-related mortality in India and other low-resourced environments.
Methods
This is a retrospective cohort study of injured patients presenting to university hospitals in India (LMIC) and the USA (HIC). The US National Trauma Data Bank (NTDB) and India’s TITCO database were used for this comparison.
The data from India were gathered from, and overseen by, a research consortium of university hospitals across the four major metropolitan areas: Apex Trauma Centre of the All-India Institute of Medical Sciences, New Delhi (north central India); Lokmanya Tilak Municipal General Hospital, and King Edward Memorial Hospital, Mumbai (western India); Seth Sukhlal Karnani Memorial Hospital, Kolkata (eastern India) and Rajiv Gandhi Hospital, Chennai (south India). The Apex Trauma Centre is a stand-alone trauma center, and the other sites are trauma units at university-affiliated teaching hospitals. These hospitals function as tertiary care facilities free to public with nominal user fees, facilitating access to care for the lower socioeconomic strata of the population. Data in India were collected by project officers via record review and direct observation in the area where trauma patients were received. The project officers could ask healthcare staff for values of parameters not entered into the patient’s records to ensure more comprehensive data collection.
Data were collected between January 2013 and December 2015 for the NTDB data and between July 2013 and December 2015 for the TITCO data. Patients with blunt or penetrating trauma, over 18 years of age, and alive on arrival to the emergency department (ED) from a transfer facility or scene were included. Patients with isolated limb injury and patients who were dead on arrival were not included during data collection in the TITCO data set and were excluded from the NTDB data set.20 Patients who died in the ED were included. Patients younger than 18 years of age, those who sustained burn injuries, and patients in the NTDB not presenting to university hospitals were excluded.
Patient characteristics, injury patterns, patient physiology, and in-hospital trauma mortality data were analyzed. Abbreviated Injury Scale (AIS) for each body region and Injury Severity Score (ISS) were used for the analysis and subanalyses. Univariate statistics, including counts, percentages, means with SDs, medians with IQRs, t-tests, Wilcoxon rank-sum tests, and Pearson χ2 tests, were used to compare patient and injury characteristics between the two groups. Multivariate logistic regression models were used to compare in-hospital risk-adjusted mortality and to conduct subgroup analyses. In-hospital mortality was the main dependent outcome variable, and location (India vs. USA) was the main independent variable. Logistic regression models controlled for age, sex, physiology, and injury severity (ISS). Statistical significance was defined as p<0.001.
All statistical analyses were performed using Stata V.16 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, Texas: StataCorp).
Results
Patient characteristics and unadjusted outcomes
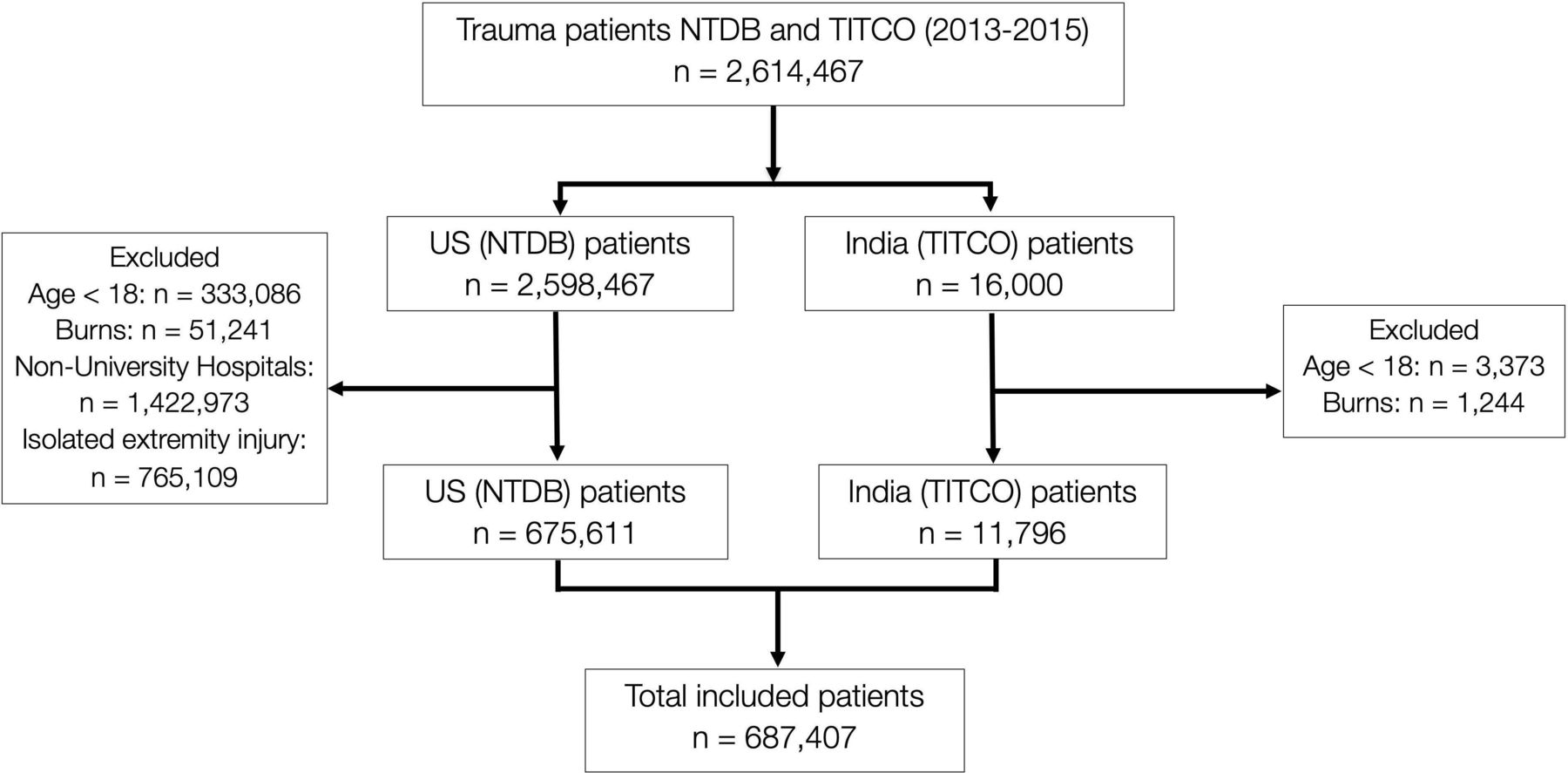
Of nearly 2.6 million trauma patients, 675 611 met inclusion criteria from the US NTDB and 11 796 from the India TITCO database resulting in a total of 687 407 patients included in the study (figure 1). Patients in India were significantly younger with a mean (SD) age of 38.7 (15.8) years compared with the USA of 48.03 (20.5) years and had significantly greater male preponderance (83.4% vs. 68.9%). In the USA, there was a significantly higher proportion of patients presenting after fall (31.3% vs. 30.4%), penetrating trauma (11.0% vs. 4.8%) and gunshot wounds (5.6% vs. 0%). Road traffic injuries include injuries associated with transportation via all motor vehicles, motorcycles, bicycles, three-wheeled vehicles, and pedestrians. There was a significantly higher proportion of patients presenting after road traffic injury (49.3% vs. 37.8%) in India (table 1).
Patient demographic, physiologic, anatomic and outcome characteristics

Patient flow diagram of NTDB and TITCO patients starting with over 2.6 million patients from the two databases and resulting in 687 407 patients. There is overlap between the exclusion categories, which were applied in parallel. The numbers presented are the true numbers for each category and not of sequential exclusion. NTDB, National Trauma Data Bank; TITCO, Towards Improved Trauma Care Outcomes.
The proportion of patients with physiologic abnormalities—respiratory with RR <10 or >29 (6.8% vs. 27.2%), circulatory with systolic blood pressure (SBP) <90 (4.1% vs. 6.3%) and neurologic with Glasgow Coma Scale (GCS) score ≤13 (16.4% vs. 44.5%)—differed significantly between the two cohorts with patients in India being more deranged in all three systems (table 1). Anatomically, there were significant differences in the proportion of patients with injuries to the different anatomic regions with the greatest difference observed for head injuries where a significantly higher proportion of patients in India presented with serious or greater (AIS score ≥3) head injuries (54.7% vs. 25.7%). While the median ISS for both groups was 9, the IQRs were significantly different when applying the Wilcoxon rank-sum test, and there was a significantly higher proportion of patients with severe injuries (ISS >25) in the US cohort (11.8% vs. 7.49%). Crude unadjusted mortality was over eightfold higher in India (23.15% vs. 2.79%) (table 1).
Adjusted mortality and subgroup analyses
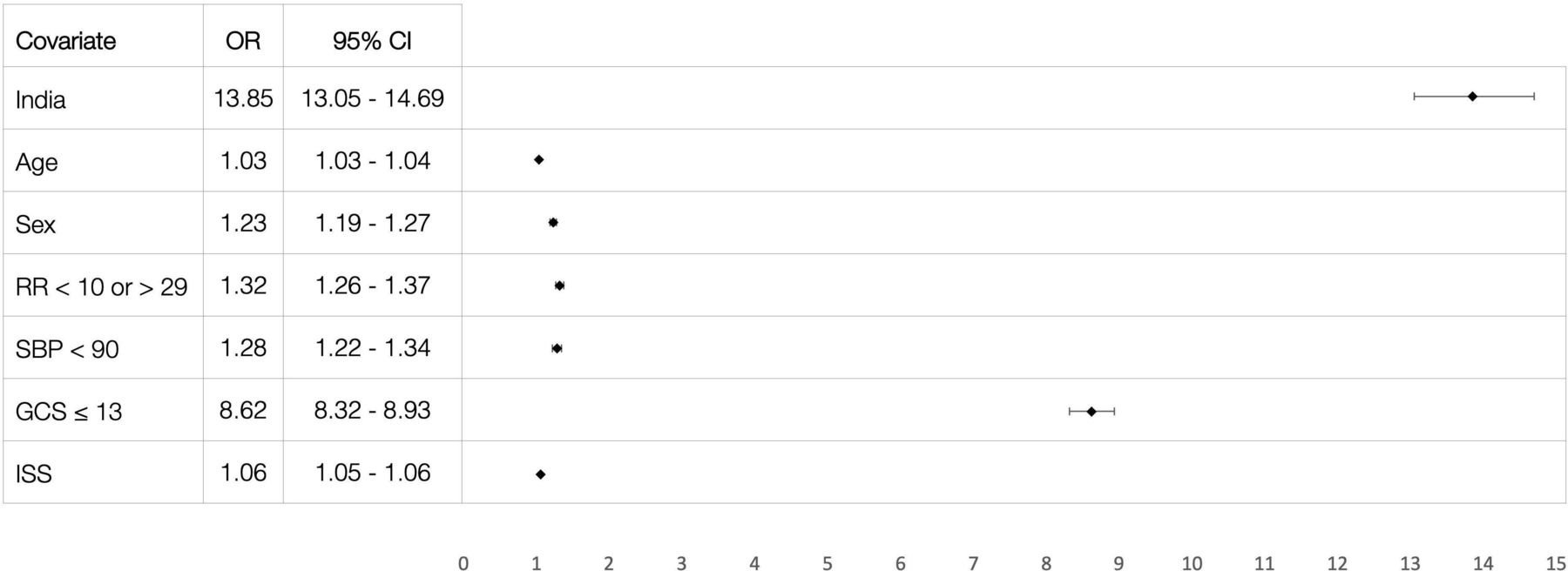
On multivariate logistic regression, age, male sex, physiologic abnormalities, and ISS were independent predictors of mortality. After adjusting for these parameters, the greatest influence on mortality was treatment location of India with an OR of 13.85 (95% CI 13.05 to 14.69). All covariates were significant (p<0.001) predictors of mortality (figure 2).

Multivariate logistic regression of independent predictors of mortality represented by a forest plot with the ORs and 95% CIs of independent predictors. All variables were significant (p<0.001). GCS, Glasgow Coma Scale; ISS, Injury Severity Score; SBP, systolic blood pressure.
Subgroup analyses comparing adjusted mortality between the India and US cohorts were performed based on age, sex, mechanism, presentation physiology, and degree of anatomic injury. In all subgroups analyzed, adjusted mortality in India was significantly higher than in the USA. The odds of mortality in India were higher for patients who were younger than 65 years, and for those with normal physiologic parameters. Given the overlapping CIs on subgroup analysis of adjusted mortality, there was no significant difference in the odds of mortality in India between males and females. Among mechanisms, the odds of mortality in India were found to be highest for road traffic injuries, which include pedestrians and drivers/passengers of all road vehicles (table 2).
Odds of mortality in India by demographic, physiologic, and anatomic characteristics
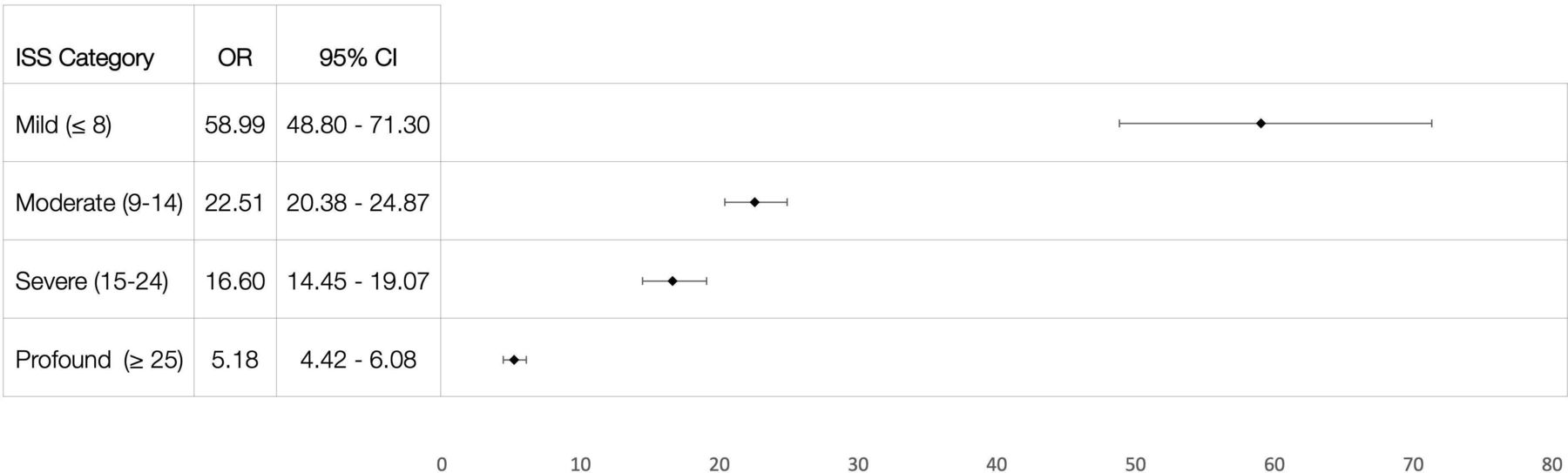
Subanalysis of anatomic injuries examined the presence of injury in each anatomic region not exclusive of other anatomic region injuries. In each AIS region, the odds of mortality were significantly higher in India except for serious to maximal facial injury. Additionally, the odds of mortality were significantly higher in India for mild to moderate injuries (AIS score 1–2), as compared with more seriously injured (AIS score 3–6), in each respective AIS region except for extremity injuries, in which the odds of mortality CIs overlap (table 2). Subgroup analysis by overall injury burden using ISS demonstrated higher odds in India for all ISS groups with the highest odds observed in the least injured (figure 3).

The odds of mortality in India from multivariate logistic regression models for each ISS category represented by a forest plot with 95% CIs. All ISS categories were significant (p<0.001).
Discussion
During the past several decades, significant progress has been made in reducing mortality in LMICs from communicable disease; however, reduction in injury-related mortality has not kept pace.21 This, combined with increased population, urbanization and mechanization, has resulted in the proportion of deaths attributable to injury actually rising.22 In contrast, in HICs, all aspects of trauma care have seen impressive improvements leading to substantial reduction in trauma-related mortality and long-term disability.
While there are studies comparing outcomes, principally mortality, between LMICs and HICs, almost all of those studies evaluate crude mortality. In the absence of adjusted mortality analysis that accounts for differences in patient populations, physiologic characteristics, and injury patterns, the true picture is unclear. More importantly, without detailed subgroup analyses evaluating the specific population and injuries contributing the most to the mortality, it is difficult to develop targeted interventions that will result in substantial reduction in trauma-related mortality in LMICs. The current study addresses this gap in knowledge by comparing adjusted mortality in an LMIC (India) and HIC (USA). Additionally, a detailed subgroup analysis identifies specific patients and injuries that could be addressed for reduction in mortality.
The independent predictors of mortality identified in the study were those that are well known—chronic physiology (age), acute physiology (abnormal values for respiratory rate, hypotension with SBP less than 90 mm Hg, and altered neurologic status with a GCS score less than or equal to 13), and magnitude of anatomic injury (AIS and ISS). After controlling for these known predictors of trauma mortality, the greatest impact on mortality was the treatment location of India. While the crude mortality was eightfold higher in India, the adjusted mortality was over 13 times higher. This difference in crude and adjusted mortality demonstrates the utility of risk adjustment for an accurate understanding of the problem. The most notable findings in subgroup analyses are that patients who were younger, with milder injuries, and normal physiologic parameters demonstrated higher odds of mortality in India. These findings seem paradoxical, and they suggest that among older, more physiologically deranged, and more severely injured patients some will die irrespective of the care provided.
A detailed analysis of the causes of mortality among both groups is beyond the scope of the current study. However, a previous study used the same TITCO data set and performed a consensus-based Delphi review to determine the preventable deaths and opportunities for improvement. In the study, almost 50% of the deaths were deemed preventable and the broad opportunities for improvement identified were: appropriate management of head injuries (23.3%); timely resuscitation and hemorrhage control (16.8%); appropriate airway management (14.3%); development and adherence to protocols (12.7%); preventing prehospital delays (10.3%); and avoiding ventilator-related complications (5.1%).12
These findings complement the risk-adjusted analysis of the current study demonstrating that the greatest odds of mortality in India were in the young, less physiologically deranged patients carrying the smallest injury burden. Both the current risk-adjusted trauma mortality study and the prior Delphi review of preventable deaths suggest that relatively low-fidelity interventions focused on standard timely trauma care and protocolized treatment pathways, as opposed to technologically complex and cost-intensive interventions, will lead to the greatest reduction in trauma-related mortality.
Organized trauma care systems save lives,23–25 and despite the human costs of injury and the existence of evidence-based and low-fidelity interventions, national and global health agendas have failed to give priority to care of the injured.26 27 Trauma care system improvement efforts can focus on guidelines for essential trauma care outlined by the WHO.13 28 While a detailed discussion of interventions is beyond the scope of the current study, focused interventions may have the greatest impact in this setting including:
Dedicated trauma training programs oriented to limited resource settings and a spectrum of care providers (specialists, physicians, advanced practice providers, clinical officers, nursing, prehospital and lay providers), which have been shown to reduce trauma morbidity and mortality, improve clinical and cost-effectiveness, and have sustained improvements in trauma care capacity in LMICs.29–34
Protocols for triage, evaluation and resuscitation, and trauma care checklists (eg, the WHO Trauma Care Checklist),35 which have demonstrably improved process and outcome measures in LMICs.36–41 This has been identified as a system-level gap in prior India trauma system assessments and reviews.10 11
Trauma quality improvement programs are an essential, low-fidelity component of successful trauma care systems,28 and have demonstrated notable improvements in mortality, structural and process measures.31 42 Systematic data collection, performance monitoring, system evaluations, and quality improvement programs are critically lacking in India.8–11
Like all studies, the current study has limitations. First, it only considers trauma patients presenting to university medical centers, and the results may not be generalizable to rural, community hospitals, or non-academic medical centers. Second, it is retrospective and, thus, subject to confounding. Third, the study only evaluates trauma patients presenting alive at a hospital and thus does not account for patient deaths from scene, transport or at transfer facilities, nor are spatiotemporal elements (travel distance and times) accounted for. And lastly, adjusted mortality for the magnitude of injury is dependent on accurate determination of ISS, which is dependent on aggressiveness of imaging to find and document even minor injuries. ISS can underestimate injury burden in limited resource settings, where imaging is less used, and when patients do not survive to the point of obtaining imaging. Further studies comparing diagnostic and therapeutic interventions are needed to more clearly identify and correlate differences in outcomes.
Conclusion
Despite these identified limitations, the current study clearly demonstrates that after adjusting for demographics, physiologic abnormalities, and injury severity, trauma-related mortality is significantly higher in India. When compared with trauma patients in the USA, the risk-adjusted odds of mortality are highest in younger patients, those with normal physiologic parameters, and patients with mild to moderate injuries. While troubling, this suggests that low-fidelity interventions focused on standard, timely trauma care and protocolized treatment pathways could result in substantial improvements for injury-related mortality in India. Additional research is needed to evaluate differences in trauma diagnostic and therapeutic interventions, and to determine which essential components of these trauma systems contribute most to the difference.
Data availability statement
TITCO data are available in a public, open access repository. NTDB data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
Data in both the NTDB and TITCO databases were deidentified, and the study was considered exempt from human subjects review by the University of Vermont Institutional Review Board (STUDY00001272).
Acknowledgments
We would like to acknowledge David Amato for assistance with data cleaning and merging of data sets.
Footnotes
Contributors NR and MM designed the data collection tools and/or monitored the data collection in India. SA and LB wrote the statistical analysis plan, and cleaned and analyzed the data. SA and AM drafted and revised the article. SA, LB, MM, NR, and AM contributed to the final edits. SA and AM accept full responsibility for the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}