

Article Figures & Data
Figures
- Figure 1
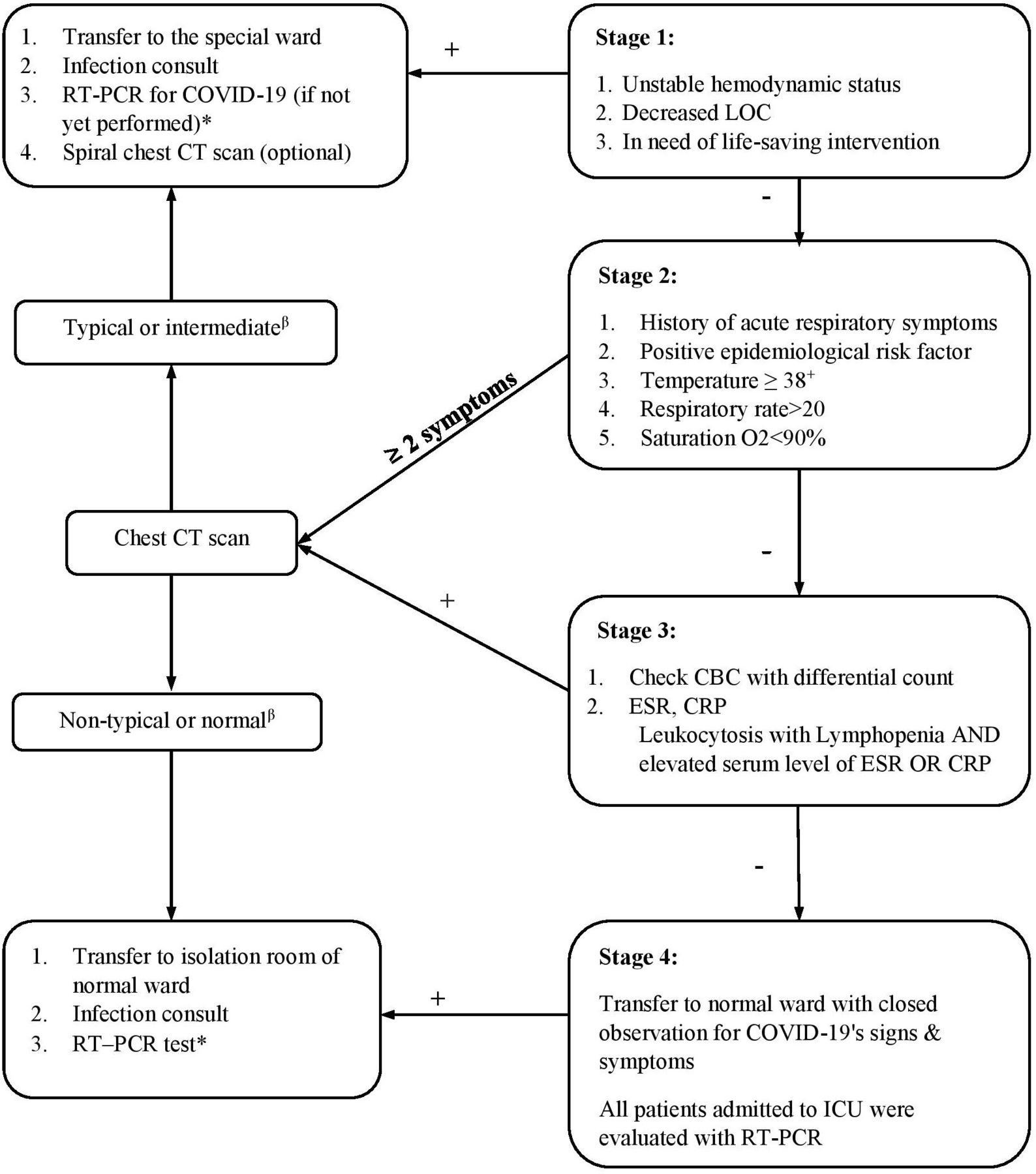
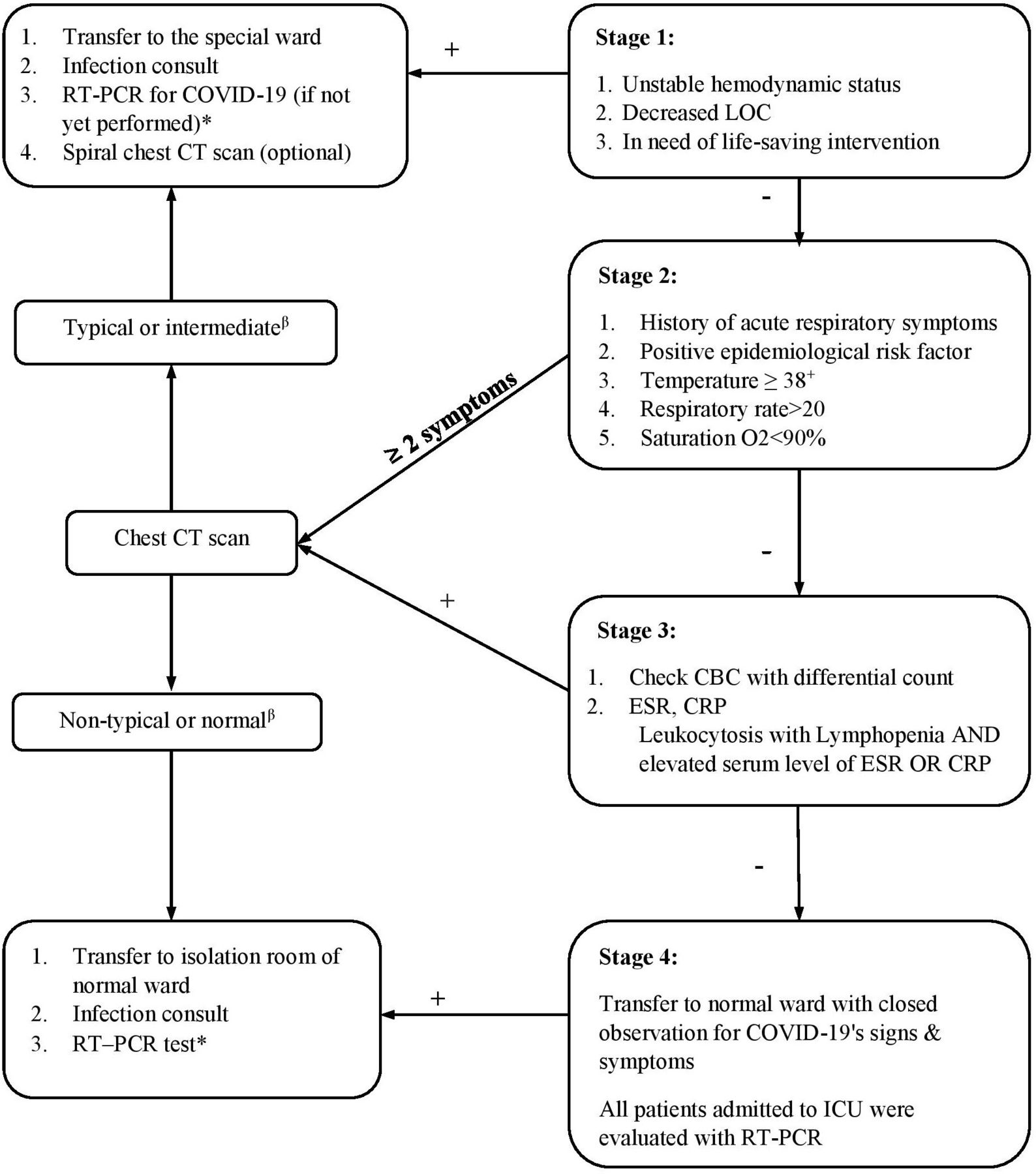
In our triage model, patients with unstable vital signs, decreased LOC, and in need of life-saving surgeries were considered suspicious for COVID-19 and transferred to special wards after proper resuscitation. In the second step, other patients who did not meet the above criteria, were assessed using their medical histories, epidemiological risk factors (as subjective parameters) and body temperature, respiratory rate (RR), and oxygen saturation (as objective parameters). In the third step, we evaluated individuals according to the obtained laboratory data for evaluating asymptomatic carriers. All other patients were transferred to regular wards and were closely monitored for signs and symptoms of COVID-19. All patients admitted to the ICU wards and those who developed COVID-19 related symptoms were also evaluated during their hospital course using RT-PCR. *A negative result was repeated 4 days later from the lower respiratory tract. **All ICU-admitted patients: evaluated by RT-PCR test. +Two times in 30 min. β, according RSNA classification. CBC, complete blood count; CRP, C-reactive peptide; ESR, erythrocyte sedimentation rate; ICU, intensive care unit; LOC, level of consciousness; RSNA, Radiological Society of North America; RT-PCR, reverse transcription-polymerase chain reaction.
Tables
- Table 1
Definition of suspicious COVID-19 cases, according to WHO, MOHME, and ECDC protocols.
Protocols Case definition WHO6 Suspected case of SARS-CoV-2 infection:
A person who meets the clinical AND epidemiological criteria:
Clinical criteria:
Acute onset of fever AND cough; OR · Acute onset of ANY THREE OR MORE of the following signs or symptoms: Fever, cough, general weakness/fatigue, headache, myalgia, sore throat, coryza, dyspnea, anorexia/nausea/vomiting, diarrhea, altered mental status.
Epidemiological criteria:
Residing or working in an area with high risk of transmission of virus: closed residential settings, humanitarian settings such as camp and camp-like settings for displaced persons; anytime within the 14 days prior to symptom onset; or · Residing or travel to an area with community transmission anytime within the 14 days prior to symptom onset; or · Working in any healthcare setting, including within health facilities or within the community; any time within the 14 days prior to symptom onset.
Probable case of SARS-CoV-2 infection:Patient who meets clinical criteria above AND is a contact of a probable or confirmed case, or linked to a COVID-19 cluster.
Suspect case with chest imaging showing findings suggestive of COVID-19 disease.
Person with recent onset of anosmia (loss of smell) or ageusia (loss of taste) in the absence of any other identified cause.
Death, not otherwise explained, in an adult with respiratory distress preceding death AND was a contact of a probable or confirmed case or linked to a COVID-19 cluster.
Confirmed case of SARS-CoV-2 infection:Person with a positive Nucleic Acid Amplification Test (NAAT).
Person with a positive SARS-CoV-2 antigen-RDT AND meeting either the probable case definition or suspect criteria A or B.
An asymptomatic person with a positive SARS-CoV-2 antigen-RDT who is a contact of a probable or confirmed case.
MOHME7 Suspicious case A person with severe febrile respiratory disease who needs to be hospitalized due to fever, cough, etc, and another pathogen to justify his disease’s symptoms is not conceivable.
Which has at least one of the following characteristics:History of travel to endemic area within 14 days before the onset of symptoms
Be one of the healthcare providers
Despite appropriate pneumonia treatments, the clinical response is inadequate, and the clinical condition is unusual and unexpected.
ECDC8 Clinical criteria
Any person with at least one of the following symptoms:
Cough
Fever
Shortness of breath
Sudden onset of anosmia, ageusia, or dysgeusia
Diagnostic imaging criteria: Radiological evidence showing lesions compatible with COVID-19
Laboratory criteria: Detection of COVID-19 nucleic acid in a clinical specimen
Epidemiological criteria
At least one of the following epidemiological links:
Close contact with a confirmed COVID-19 case in the 14 days before the onset of symptoms
Having been a resident or a staff member, in the 14 days before the onset of symptoms, in a residential institution for vulnerable people where ongoing COVID-19 transmission has been confirmed
Case classification
Possible case:
Any person meeting the clinical criteria
Probable case:
Any person meeting the clinical criteria with an epidemiological link
OR
Any person meeting the diagnostic criteriaConfirmed case:
Any person meeting the laboratory criteriaCOVID-19, coronavirus disease 2019; ECDC, European Centres for Disease Control; MOHME, Iranian Ministry of Health and Medical Education; RDT, rapid diagnostic test; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
- Table 2
Demographic data and clinical histories of the suspicious cases (n=132)
Variables RT-PCR +ve (n=30) RT-PCR −ve (n=102) P value Sex; number (%) Male 24 (80%) 78 (76.5%) – Female 6 (20%) 24 (23.5%) – M/F 4 3.25 0.68 Nationality; number (%) Iranian 27 (90%) 92 (90.2%) 0.97 Non-Iranian 3 (10%) 10 (9.8%) COVID-19 related history; number (%) Close contact 7 (23.3%) 5 (4.9%) 0.002 Fever 10 (33.3%) 32 (31.4%) 0.83 Cough 6 (20%) 11 (10.8%) 0.18 Respiratory distress 16 (53.3%) 13 (12.7%) <0.001 Neurological symptoms* 5 (16.7%) 6 (5.9%) 0.06 Abdominal pain 3 (10%) 0 0.01 Anorexia 1 (3.3%) 10 (9.8%) 0.22 Past medical history; number (%) Cancer 2 (6.7%) 0 0.05 DM 3 (10%) 6 (5.9%) 0.43 Chronic anemia 1 (3.3%) 0 0.22 Cardiac disease 3 (10%) 7 (6.9%) 0.56 CKD 0 1 (1%) 1.0 Asthma 0 2 (2%) 1.0 COPD 2 (6.7%) 0 0.05 HTN 4 (13.3%) 8 (7.8%) 0.35 Hospital course; number (%) Intubation 11 (36.7%) 38 (37.3%) 0.95 Mortality 5 (16.7%) 11 (10.8%) 0.38 ALOS (days); mean (SD) 8.1 (5.6) 10.66 (13.66) 0.63 *Defined as the presence of any of the followings: anosmia, dysgeusia, ageusia.
ALOS, average length of hospital stay; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; HTN, hypertension; M/F, male to female ratio; RT-PCR, reverse transcription-polymerase chain reaction; −ve, negative; +ve, positive.
- Table 3
Diagnostic capability of available protocols in detecting COVID-19 among trauma patients
Protocols RT-PCR Sensitivity (%) Specificity (%) +ve (n=30) −ve (n=610) WHO Suspicious 4 0 13.3 100 Non-suspicious 26 610 MOHME Suspicious 7 1 23.3 99 Non-suspicious 23 609 ECDC (possible) Suspicious 28 64 93.3 89.5 Non-suspicious 2 546 ECDC (probable) Suspicious 7 1 23.3 99 Non-suspicious 23 609 Our stepwise triage system Suspicious 28 59 93.3 90.3 Non-suspicious 2 551 ECDC, European Centre for Disease Control and Prevention; MOHME, Iranian Ministry of Health and Medical Education; RT-PCR, reverse transcription-polymerase chain reaction; +ve, positive; −ve, negative.
- Table 4
Frequency of positive clinical and laboratory findings in suspected patients (n=130)
Stages Detected patients (%) RT-PCR (n=30) Stage 1 54 (40.9%) 17 (56.7%) 1. Decrease in LOC 24 (18.2) 7 (23.3%) 2. Unstable hemodynamics 32 (24.2) 9 (30%) 3. Life-saving surgery 5 (3.8%) 1 (3.3%) 4. Both 1 and 2 5 (3.8%) 3 (10%) 5. Both 1 and 3 2 (1.5%) 1 (3.3%) Stage 2 40 (30.3%) 9 (30%) 1. History of respiratory symptoms 25 (18.9%) 2. Epidemiological factors 9 (6.8%) 3. Fever 20 (15.2%) 4. RR >20 21 (15.9) 5. Sat O2 51 (38.6%) Stage 3 14 (10.6%) 0 (0%) 1. Leukocytosis 23 (17.4%) 2. Lymphopenia 27 (20.5%) 3. High ESR 13 (9.8%) 4. High CRP 23 (17.4%) Stage 4 22 (16.7%) 2 (6.7%) 1. Fever 2 (1.5%) 2 (6.7%) CRP, C-reactive peptide; ESR, erythrocyte sedimentation rate; LOC, level of consciousness; RR, respiratory rate; RT-PCR, reverse transcription-polymerase chain reaction.




{kind=link}