

Abstract
Objective There is a paucity of evidence about traumatic injuries and their sequelae sustained due to equestrian injuries nationally.
Methods Retrospective study analyzing National Trauma Data Bank data from 2007 to 2016. Variables collected included age, sex, race, payer status, Injury Severity Score (ISS), hospital length of stay, Glasgow Coma Scale, systolic blood pressure (SBP) at presentation, discharge disposition, and mortality. Patient data were analyzed by anatomic region.
Results The most frequent type of injury was in the thorax, but head and neck injuries produced the highest mortality. Increased ISS and an SBP of less than 90 mm Hg were also significant predictors of mortality.
Conclusions The risk of hospital admission from equestrian injuries is higher than football, motor vehicle racing, and skiing. Preventive measures and campaigns should be instituted to highlight safety practices and the use of personal protective equipment while on horseback either for sports, leisure, or work.
Level of evidence Level IV. Retrospective study.
Introduction
Humans have been domesticating horses for at least 5500 years.1 Equus ferus caballus helped revolutionize human society and were instrumental in the advancement of fields such as agriculture and transportation. Our relationship with horses has continued to evolve over the years, and they are now commonly used for both work and recreational activities. Although domesticated, horses’ behavior may be unpredictable. Their large size and strength can generate significant amounts of mechanical kinetic energy which can be transferred to an equestrian, resulting in unfortunate accidents. According to the Centers for Disease Control and Prevention, each year in the USA, more than 30 million people participate in equestrian activities.2 Although accurate estimations are confounded by unidentified injuries that do not make it to hospitals, equestrian accidents are more commonly being recognized as a contributory source of sports-related injuries, especially with respect to traumatic brain injuries (TBI).3 TBIs might be worsened when you consider that more experienced riders were less likely to wear a helmet, although at most risk for injuries requiring hospitalization or causing permanent disability.4
There is a lack of evidence focused on traumatic injuries sustained due to equestrian injuries nationally. Most have focused on injuries sustained in a small geographical region and may lack generalizability to a national population. Furthermore, there have been few studies that provide insight into the sequelae of equestrian-related trauma. This study aims to uncover and report national-level data about equestrian-related trauma using the National Trauma Data Bank (NTDB). The NTDB is the largest aggregation of US trauma registry data and is the national standard for exchanging trauma registry data.5 Using this data bank, a 10-year review (2007–2016) was conducted to identify injuries sustained while horseback riding in the adult population. This retrospective analysis characterizes mortality rates, hospital length of stay (LOS), intensive care unit (ICU) LOS, ventilator days, and emergency department (ED) disposition of equestrian-related trauma injuries. Our goal was to reveal the demographic and epidemiological data that will allow for the development of targeted prevention strategies.
Methods
Data source and study population
This study collected data from the NTDB during a 10-year period between 2007 and 2016. The NTDB collects data from patients who present to all level I and level II trauma centers. Level III and IV trauma centers can participate in the data bank voluntarily. All patient data are deidentified and aggregated. Patients 18 years of age and older involved in equestrian-related injuries were analyzed. Equestrian injuries were uncovered from the NTDB using the appropriate external cause of injury code (E-code) as defined in their data dictionary.6 The data set was stratified by the type of insult sustained using the appropriate International Classification of Diseases-9th/10th Revision (ICD-9/ICD-10) codes. Injuries were aggregated into categories based on the anatomic location of the injury. Patients’ results with missing or incomplete data were excluded from the analysis.
Study variables
Patients were classified based on demographic data such as age, sex, race, and payer status. Variables extracted from the NTDB also included Injury Severity Score (ISS), hospital and ICU LOS, and admission Glasgow Coma Scale (GCS). Other variables that were obtained from the NTDB were hospital and ED discharge disposition. ED systolic blood pressure (SBP) was also analyzed with <90 mm Hg being considered the threshold for shock. Mortality data were obtained from ED and hospitalized patient data and analyzed by injury type.
Statistical analyses
Continuous variables were reported as mean with SDs, while non-continuous variables were reported as frequencies with percentages. Statistical analyses were performed via χ2 test or Fisher’s exact test for categorical variables. Analysis of variance (ANOVA) or Kruskal-Wallis test was used for continuous variables. The use of the ANOVA test was dictated by the Shapiro-Wilk test of normality. The Fisher’s exact test was used instead of the χ2 test, where a cell count was less than 5. A multivariable logistic regression was used to assess the association between death and injury type, and the analysis was adjusted for race, payer status, age group, and severity of the injury. ORs, CIs, p values, means, SDs, proportions (p), and sample sizes (n) were reported. A p value <0.05 corresponds to results that were statistically significant at a 95% confidence level. Also, when 1.96 times SD is less than the corresponding mean, the finding was considered statistically significant at a 5% level of significance. Data processing and analysis were performed using Stata/MP V.16.1 (StataCorp, College Station, Texas, USA).
Results
Demographics and injury distribution
During the 10-year study period (2007–2016), 45 671 patients were retrieved from the NTDB using the E-codes related to equestrian injuries. A total of 20 880 patients were omitted due to missing or incomplete information, leaving 24 791 included in the analysis. Patients’ mean age (±SD) of the studied population was 46.85 (±15.33), with an almost equal proportion of males and females (males: 50.53%) and a majority of Caucasians (61.62%). The most common injuries recorded were in the thoracic region with 9189 (37.07%) patients (table 1). Extremity injuries occurred in 6560 (26.46%) patients whereas 5689 (22.95%) sustained head injuries. Abdominal injuries were the least common, with only 3353 (13.53%) experiencing this type of injury. Most patients were insured (69.94%), with a small portion of patients (14.75%) being uninsured. A majority of patients, 23 619 (95.27%), presented to the ED with an SBP ≥90 mm Hg. Only 347 (1.40%) of patients presented with an SBP <90 mm Hg, our threshold for a hemodynamic shock.
Statistical summary of variables for equestrian-related injuries in adults
Severe neurological impairment classified as a GCS score of 3–8 on presentation was observed in 888 (3.58%) patients. Within the severe impairment group, head and neck injuries were the most likely cause, occurring in 706 patients. Moderate impairment (GCS score 9–12) occurred in only 258 (1.04%) of patients. In the cohort, 21 917 (88.41%) patients presented with a GCS score between 13 and 15. Due to the categorization of GCS, it is impossible to segregate those with no impairment (GCS score 15) from those with some mild form of cognitive impairment (GCS score 13–14). However, we observed that 4508 (20.5% of 21 917) patients from the normal to mild GCS impairment group had a head and neck injury.
Patient ISS values were ranked mostly in the minor or moderate ISS subgroups (33.28% and 43.59%, respectively) but resulted in a large proportion of admissions to the hospital (88.19%). Half of the admitted patients were sent to a floor bed (50.05%), with 28.32% being sent to an ICU. The operating theater (9.82%) was the third most likely destination for patients with equestrian injuries being evaluated in the ED. Equestrian injuries that presented to the ED had a low likelihood (5.15%) of being discharged home from the ED.
Inpatient characteristics and mortality
The mean hospital LOS was 4.46 days (SD 5.27; table 2). Patients spent an average of 3.96 days (SD 5.17) in the ICU and a mean of 5.80 days (SD 7.06) on a ventilator. Patients admitted to the ICU with head and neck injuries required 1.54 more days (95% CI 0.13 to 9.96; p<0.05) on the ventilator as compared with patients with extremity injuries. Likewise, ICU patients with head and neck injuries had 3.05 more days on the ventilator (95% CI 1.53 to 4.58; p<0.001) than patients with abdominal injuries. However, the difference in ventilator days between head and neck injuries and thoracic injuries did not achieve statistical significance (0.63, 95% CI −0.23 to 1.50; p>0.05).
Distribution of variables for adult equestrian by injury type
The 50–59 age group was found to be most likely to present to trauma centers, accounting for 5939 (26.58%) injuries. Older riders, those belonging to the 60+ age group, came in second with 4883 (21.85%) incidents in the period analyzed. The 40–49 age group came in third with 4568 (20.44%) reported events. Patients in the youngest category, the 18–29 age group, accounted for 4009 (19.94%) injuries. Finally, the 30–39 age group was the least likely age group to be reported in equestrian injuries accounting for 2946 (13.18%) patients. Table 2 further illustrates a breakdown of the total injuries per age group and anatomic region.
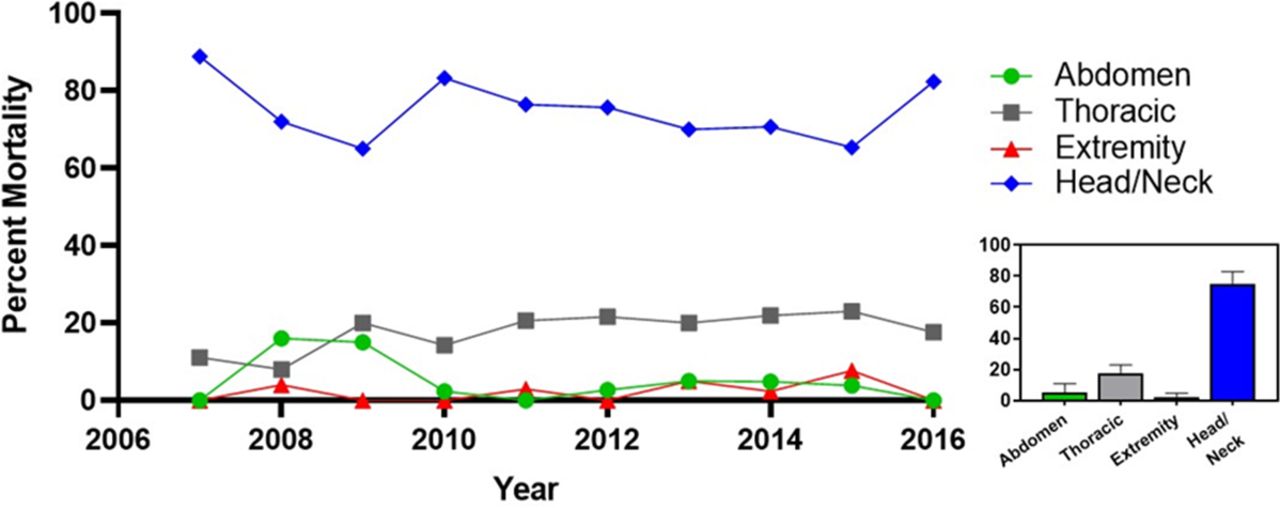
For the patients who survived their hospital stay, 14 096 (56.86%) were discharged home without additional services, and 1747 (7.05%) were discharged/transferred to a rehabilitation or skilled nursing facility. On the other hand, 320 deaths resulted from equestrian-related injuries over the study period. Head and neck injuries were the leading cause of mortality, with 237 (74.83%) deaths recorded (figure 1). Thoracic injuries were second with 59 (18.44%), and abdominal injuries were causing the third highest number of deaths, with 17 (5.31%). Finally, extremity injuries led to the least number of deaths, with 7 (2.19%) patients dying to their injuries. Using extremity injuries as a reference, patients were more likely to pass away due to head and neck trauma (OR 44.07, 95% CI 21.30 to 91.19, p<0.001) than from abdominal injuries (OR 5.8, 95% CI 2.45 to 13.72, p<0.001) or thoracic injuries (OR 5.8, 95% CI 2.75 to 12.52, p<0.001). Unsurprisingly, as ISS increased, so did the likelihood of death. When compared with minor ISS, moderate ISS led to a doubling the risk of mortality (OR 2.64, 95% CI 1.38 to 5.05, p<0.01), severe ISS increased the risk of mortality eight times (OR 8.21, 95% CI 4.28 to 15.74, p<0.001), and very severe injuries increased the risk of mortality by more than 100 times (OR 141.71, 95% CI 78.62 to 255.42, p<0.001). If the patients arrived to the ED with an SBP <90 mm Hg, the patients were 23 times more likely to die compared with patients with an SBP ≥90 (OR 23.37, 95% CI 16.95 to 32.23, p<0.001).
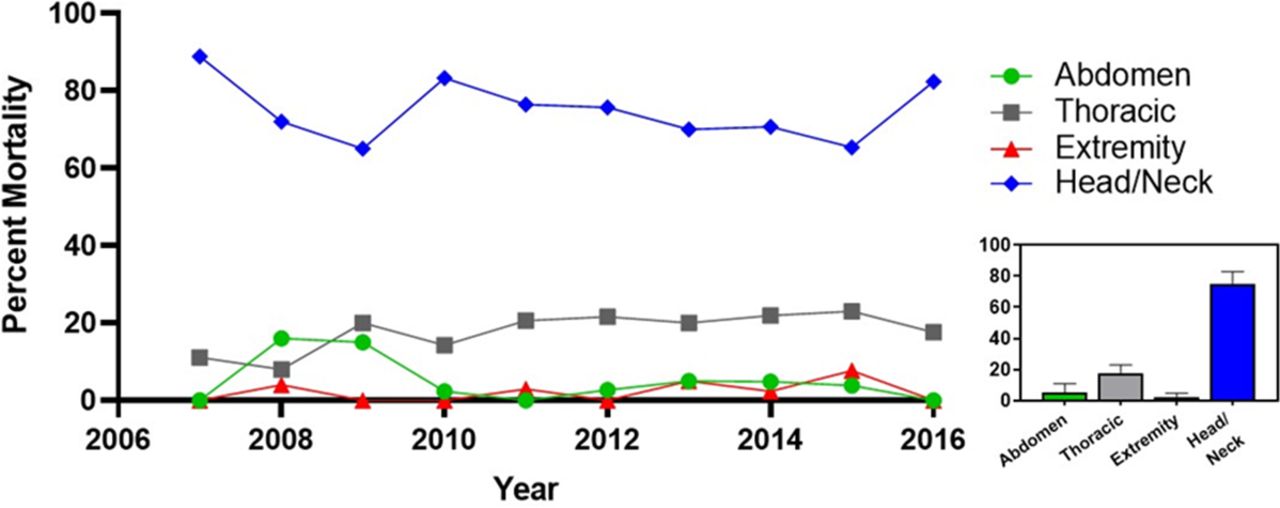
Mortality due to equestrian-related injuries. All equestrian-related injuries reported per year in the National Trauma Data Bank (NTDB) were subdivided by anatomic region clearly revealing that head and neck injuries lead to the highest mortality during the 10 years analyzed. Inset on the right shows the mean (SEM) of equestrian-related injuries across the 10 years, with head and neck injuries showing the highest average mortality and extremity injuries the lowest.
Discussion
Equestrian-related injuries are a frequently ignored public health issue due to the lack of a national survey. Previous studies have characterized the mechanisms of injury or injury patterns for equestrian injuries7 8; however, these were local retrospective studies. Furthermore, previous studies did not include any inpatient data that would assess inpatient and acute outcome data such as ICU LOS, ventilator days, and mortality rates after equestrian injuries. To our knowledge, this study is the first to characterize the inpatient characteristics and outcomes of adults involved in equestrian injuries from a large national sample during a 10-year period.
Equestrian injuries presenting at level I and level II trauma centers found that over 88% of patients showed only mild or no neurological impairment (GCS score 13–15). Severely impaired patients were second but accounted for only 3% of total admissions. Of all patients who presented to the hospital, 88% were admitted. This mirrors previous findings showing the proportion of admissions from equestrian injuries was 3.5 times higher than data reported for motorcycle riding.9 When taken together, these data suggest that the dangers of equestrian activities have been severely underappreciated. When controlled for hours of activity, horseback riding resulted in a higher proportion of hospital admission than other higher risk activities like skiing.10 One of the best examples of a severe equestrian injury is the broadly publicized accident that the American actor Christopher Reeve sustained in 1995 during a competition. His horse abruptly stopped, resulting in Reeve flying over a barrier and landing head first. Reeve was an experienced rider and was wearing a helmet when the accident happened, but this was still not enough to protect him from the force of the impact that led him paralyzed for the rest of his life.11 12 While many horses used in sports are well trained, the interaction with a large animal is not exempt from unpredictable behavior and/or unforeseen environmental circumstances leading to accidents.
Across the injury types analyzed, several important trends were noted. First, head and neck injuries were the largest contributor to mortality in equestrian injuries across all 10 years surveyed. Not surprisingly, head and neck injuries were also significantly associated with longer ICU LOS and more ventilator days. Head and neck injuries were also associated with a ninefold increase in the risk of death. This finding coincides with previous data indicating greater mortality from head and neck injuries in equestrian-related accidents.13 Our study adds to the evidence suggesting that using protective equipment such as helmets in equestrian activities could provide a benefit in reducing injuries. Helmet use has not been widely adopted in the horse riding community, given the lack of public health campaigns that specifically target casual riders and people who use horses for work. Studies have shown that a large fraction of riders involved in equestrian injuries were not wearing helmets at the time of their accident.14 It stands to reason that raising awareness of the possible injuries and increasing preventive measures to protect against head injuries would significantly reduce mortality.
Furthermore, little work has been done to quantify the real costs of equestrian injuries. Although overall death numbers are low,15 previous work has shown that the long-term rehabilitation costs to treat these injuries may be high.16–18 Further research looking into the epidemiology and true financial burden of these injuries is warranted.
Our study also uncovered demographic data, which revealed men and women were injured at the same rate. This goes against several studies that have claimed that women are injured more often in equestrian-related injuries.19–21 This finding would suggest that both sexes are susceptible to injuries and that the current prevention efforts should be focused on both sexes. Some studies have suggested targeting safety efforts on female19 and young riders22; however, improved safety outcomes are warranted if prevention efforts are more generalized.
This study is not without limitation. The retrospective analysis included only injured patients in equestrian-related accidents that presented to US trauma centers that report data to the NTDB. This likely excludes rural hospitals or other small community hospitals which do not contribute to the NTDB. We did not have access to unreported equestrian-related injuries or injuries that were not coded appropriately for inclusion into the NTDB database, which may have led to underestimating the true prevalence of equestrian-related injuries in the USA.
Although much care was used in selecting the appropriate ICD-9, ICD-10, and E-codes to query the NTDB, it must be noted that inaccurate or missing data from incorrectly coded patients may have caused the underestimation of different types of injuries in our analysis. Despite these limitations, the NTDB remains a powerful tool in uncovering patterns and prevalence in different traumatic presentations and remains the most extensive wide-scale trauma databank available for US trauma centers.
Conclusion
Horseback riding is immensely popular among Americans. It is estimated that 1 in 63 US persons come into contact with horses each year.23 Although they are used for both leisure and work, the real impact of equestrian-related injuries can often be ignored.16 24 As TBIs have become more apparent in the mainstream media due to reports of chronic traumatic encephalopathy in football players,25 it is imperative to discuss the dangers of equestrian-related activities while underscoring the importance of safe riding. Many public health initiatives have focused on making sure that participants wear helmets during bicycle and motorcycle riding.26 27 Furthermore, research funding has mirrored public interest as the National Football League pledged millions of dollars in grant funding to launch the Head Health campaign.28 They are hoping to define the brain injuries that occur during play29 and create new helmet prototypes that will protect the brains of athletes.30 31
Interestingly, hospital admission risk from horseback riding is higher than football, auto and motorcycle racing, and skiing.32 Recently, some attention has been paid by equestrian sporting agencies to the use of protective equipment to prevent injuries, especially as it relates to concussion and brain injuries33 34; however, very few public health campaigns have focused on preventing injuries in riders using horses for leisure and work. This is in stark contrast to the popularity of riding these animals. We suggest that preventive measures and campaigns should be instituted to highlight safety practices. Implementing the consistent use of personal protective equipment, such as helmets and vests, will provide added protection to all riders (working or leisure) while on horseback. It is also imperative that medical professionals examine patients injured during horseback riding for head and neck injuries as these contribute to the highest mortality. Together, awareness of injury patterns, we can continue to enjoy this popular sport while simultaneously reducing the number of severe injuries.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data were derived from the National Trauma Data Bank from the American College of Surgeons. The data sets used herein can be obtained by written request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the University of Texas Rio Grande Valley Institutional Review Board under the exempt category.
Footnotes
Presented at 16th Annual Academic Surgical Congress. Abstract number ASC20210800.
Contributors JJS conceived and designed the analysis, contributed the data and supervised the project. DF performed the data analysis and prepared the tables. KM and JL wrote the initial draft of the article and helped in the interpretation of data. AT-R contributed to the writing, and edited the article and figures.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JJS is employed by Renaissance Medical Foundation, the medical group that provides clinical services to DHR Health.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}