

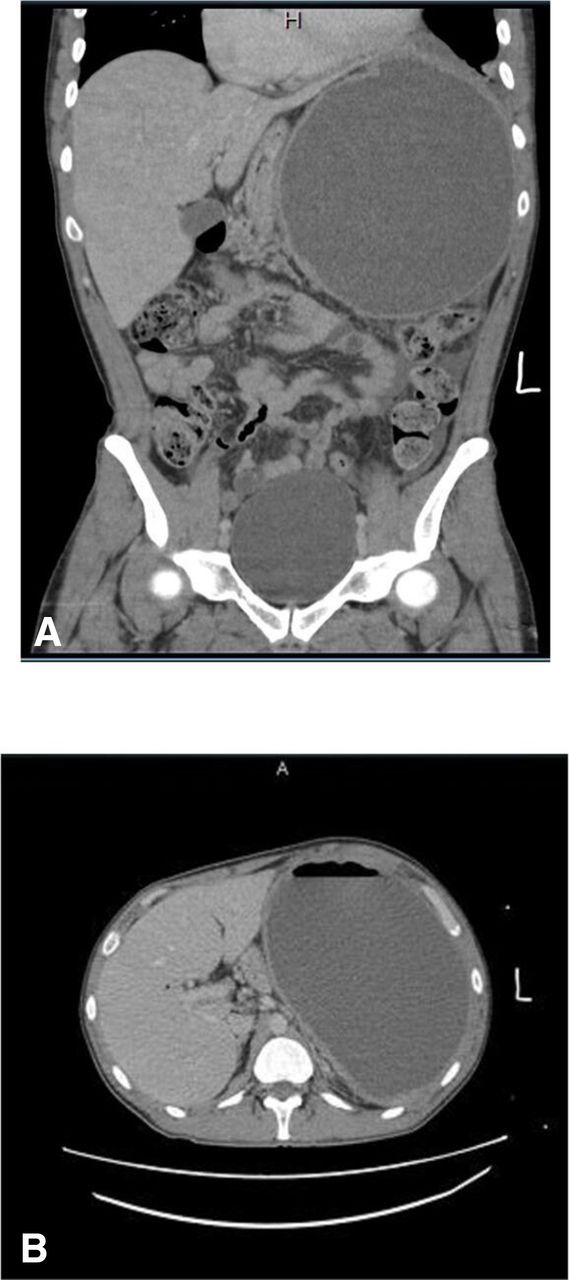
A patient in his 30s with a history of intravenous drug abuse presented to the hospital after a motor vehicle collision. The patient sustained a low-grade splenic laceration (American Association for the Surgery of Trauma (AAST) grade 2) with concern for possible active extravasation of contrast on CT of the abdomen. The patient had normal hemodynamics; however, given the concern for extravasation of contrast, a selective angiogram was performed which confirmed a small area of contrast extravasation of the lower pole. A distal splenic artery angioembolization was performed on two-thirds of ordered arterial vessels with polyvinyl acetate particles with good hemostasis. The patient recovered and was discharged home without complication. Three months later, the patient returned with abdominal distension and constant left upper quadrant pain that radiated toward the left shoulder. The patient reported feeling some abdominal pain since discharge from the hospital; however, the patient did not seek attention. On examination, the patient was afebrile, with normal hemodynamics. The abdomen was distended and tender, without guarding, particularly in the left upper quadrant. Notable labs included a white cell count of 12.9×10∧9/L. Repeat imaging studies were performed (figure 1A,B); CT abdomen with contrast revealed a large, encapsulated air and fluid collection in the spleen measuring 20.4×14.1×20.5 cm; trace left pleural effusion with atelectasis and diffuse mesenteric edema. Given the history of trauma, a post-IR splenic hematoma was suspected with possible superinfection.

(A, B) Splenic abscess with mass effect on adjacent organs.
What would you do?
Laparoscopic splenectomy
Open splenectomy
Percutaneous drainage
Antibiotic therapy
What we did and why?
C. Percutaneous drainage
Percutaneous drainage was performed with multiple liters of purulent non-bloody fluid drained. The patient’s course in the hospital was uneventful showing no significant signs of infection. Fluid culture showed rare white cells, 2+ growth moderate Gram-positive bacilli, and was positive for Actinomyces sp only. Intravenous antibiotic therapy was started but the patient chose to leave against medical advice.
Splenic artery embolization (SAE) is used for management of stable patients with AAST grade III–V splenic injury or contrast blush on CT of the abdomen or large amount of hemoperitoneum. Patients with focal vascular injury are managed with distal splenic artery embolization whereas proximal splenic artery embolization is more appropriate for patients with multifocal injury. Infection and abscesses are rare complications after SAE and routine antibiotic therapy is not necessary after the procedure. Typically, the presentation can be acute or delayed, the etiology is due to mixed organisms and the management involves splenectomy. Symptoms and signs include fever, leukocytosis, left upper quadrant pain, and left-sided pleural effusion.
This is the first case report of an afebrile patient who underwent percutaneous drainage and fluid culture revealed isolated Actinomyces sp. This case highlights a slow, indolent intra-abdominal Actinomyces infection and the importance and spectrum of infections possible from intravenous drug use. The microorganisms are Gram-positive, anaerobic, branching bacilli normally found in the oral cavity, colon, and female urogenital tract. There remains some debate whether angiography leads to postinterventional splenic abscesses.
Footnotes
Contributors Study concept, literature review, article writing: AQ. Critical reviews and revisions: all authors. Supervisor: MK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}