

Abstract
Objectives The Tactical Combat Casualty Care (TCCC) guidelines detail resuscitation practices in prehospital and austere environments. We sought to review the content and quality of the current TCCC and civilian prehospital literature and characterize knowledge gaps to offer recommendations for future research.
Methods MEDLINE, EMBASE, CINAHL, and Cochrane Central Register of Controlled Trials were searched for studies assessing intervention techniques and devices used in civilian and military prehospital settings that could be applied to TCCC guidelines. Screening and data extraction were performed according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Quality appraisal was conducted using appropriate tools.
Results Ninety-two percent (n=57) of studies were observational. Most randomized trials had low risk of bias, whereas observational studies had higher risk of bias. Interventions of massive hemorrhage control (n=17) were wound dressings and tourniquets, suggesting effective hemodynamic control. Airway management interventions (n=7) had high success rates with improved outcomes. Interventions of respiratory management (n=12) reported low success with needle decompression. Studies assessing circulation (n=18) had higher quality of evidence and suggested improved outcomes with component hemostatic therapy. Hypothermia prevention interventions (n=2) were generally effective. Other studies identified assessed the use of extended focused assessment with sonography in trauma (n=3) and mixed interventions (n=2).
Conclusions The evidence was largely non-randomized with heterogeneous populations, interventions, and outcomes, precluding robust conclusions in most subjects addressed in the review. Knowledge gaps identified included the use of blood products and concentrate of clotting factors in the prehospital setting.
Level of evidence Systematic review, level III.
Introduction
The Tactical Combat Casualty Care (TCCC) guidelines were developed in 1996 for the US Special Operations Forces to provide guidance for battlefield trauma care.1 Historic military medical data were reviewed and identified the most common and preventable causes of death on the battlefield: hemorrhaging extremity wounds, tension pneumothoraces and obstructed airways.1 Furthermore, the guidelines consider the added challenges of providing prehospital trauma care in an active military environment, such as delayed evacuation, poor visibility, and limited access to medical supplies.1 2 These factors inspired the five MARCH components within the TCCC guidelines: (1) massive hemorrhage control; (2) airway management; (3) respiratory management; (4) circulation; and (5) hypothermia prevention.1
Interventions such as tourniquets, hemostatic dressings, cricothyrotomy, needle decompression, fluid/blood product administration, and thermal blankets have been assessed in austere environments to expand the TCCC guideline evidence base.1 This evidence base is reviewed monthly by the Committee on TCCC to identify MARCH interventions currently being used or any that with potential applicability to prehospital environments.2 While these interventions are regularly reviewed, the overall body of literature is infrequently evaluated. Gap analyses are scarce. In addition, a review conducted by Martin and colleagues highlighted gaps in battlefield casualty care research, including non-operative interventions for non-compressible truncal hemorrhage, the optimization of blood products and their storage, and factor concentrates and other alternative products for hemostatic resuscitation.2
To our knowledge, no comprehensive knowledge synthesis describing the content and quality of current literature on the MARCH components of the TCCC guidelines has been performed. We sought to describe the current body of literature, evaluate its quality, identify gaps or potential limitations that exist within the TCCC guidelines, and offer recommendations for future research.
Methods
This is a systematic review conducted to identify and synthesize the scholarly research on TCCC procedures and techniques in the military and civilian settings. The review focuses on TCCC principles to identify gaps in research and to provide evidence for practice, policymaking, and future research. This systematic review was reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.3
Study eligibility criteria
Experimental (randomized controlled trials (RCTs), quasi-RCTs, and non-RCTs), quasiexperimental (controlled before-after studies and interrupted time series), and observational (cohort and case–control) studies were eligible if they examined prevention, diagnosis, or treatment for traumatic injuries in adults aged >16 in combat or non-combat prehospital settings. The interventions and outcomes of interest were those associated with the MARCH components within the TCCC guidelines.4 We focused on prehospital interventions; however, eligibility was extended to include interventions performed in hospital with potential prehospital applicability. This included innovative technologies such as blood product storage and warming techniques, medical evacuation (MEDEVAC) technologies, and new devices or techniques for prehospital surgical care. Outcomes were considered as reported by each included study.
Identification and selection of studies
A comprehensive literature search was run in Ovid MEDLINE (online supplemental table 1), Ovid MEDLINE Daily, Ovid MEDLINE In-Process & Other Non-Indexed Citations, Ovid MEDLINE Epub Ahead of Print, CINAHL (EBSCOhost), Ovid EMBASE, and Cochrane Central Register of Controlled Trials between January 1, 2001 and December 13, 2019. The literature search started in 2001 after an increase in research conducted in military settings after the September 11, 2001 terrorist attack. Non-English publications were excluded due to resource and time constraints.
Supplementary data
Data collection and study appraisal
After a calibration exercise, all literature search results were screened independently by two reviewers. The same strategy was used for data abstraction and quality appraisal of included studies. Quality appraisal was conducted using the Cochrane Effective Practice and Organisation of Care risk of bias tool for experimental and quasiexperimental studies,5 the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2)6 for diagnostic studies, and the Newcastle-Ottawa Scale (NOS)7 for cohort and case–control studies.
Synthesis of results
The data were first synthesized descriptively, reporting study and participant characteristics, quality appraisal results, and outcome frequencies across the included studies. Included studies were heterogeneous in populations, interventions, outcomes, and methodologies; therefore, a meta-analysis of the results was not conducted.
Results
Included studies
The search identified 13 857 titles and abstracts. After duplicate removal, 11 262 records were eligible for screening. After assessing titles and abstracts, 528 potentially relevant records were selected for full-text review. Figure 1 outlines the reasons for study exclusion. Table 1 outlines the characteristics of included studies; from these, 62 articles fulfilling the eligibility criteria were included (n=62 352 patients): 5 RCTs (n=773), 54 observational cohorts (n=59 227), and 3 observational case–control designs (n=2352).
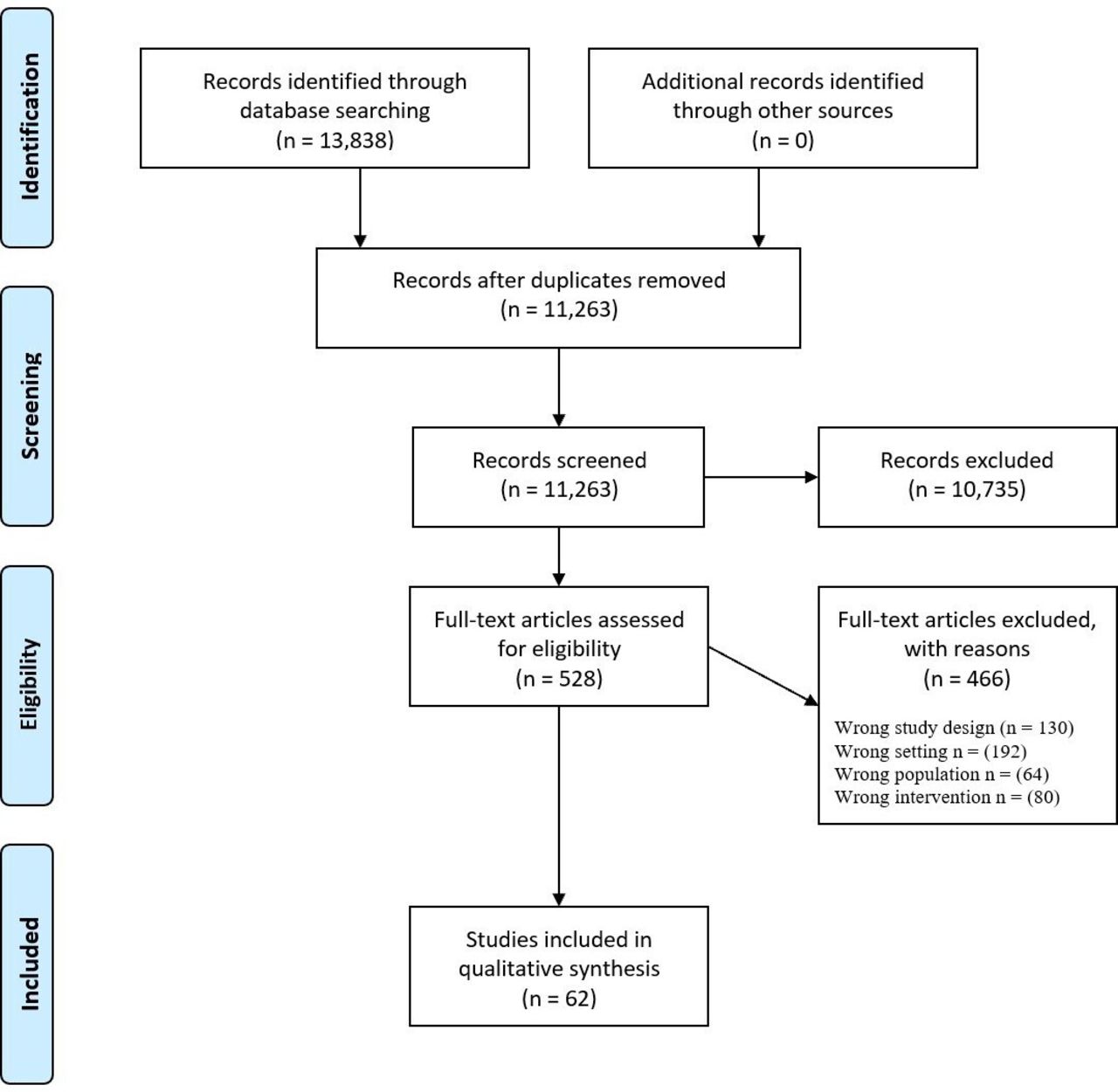
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Study characteristics
Results are reported according to the evidence-based literature identified across the databases searched. The mean±SD age, percentage male sex, and Injury Severity Score across all studies were 33.6 (±7.8) years, 85.9% (±15.1), and 28.4±17.1, respectively. Below, we summarize the findings of these studies according to the MARCH components. Detailed information about design, participants, interventions, and outcomes of each included study is presented in online supplemental table 2.
Supplementary data
Main findings of included studies
Massive hemorrhage control
Seventeen studies8–24 describing interventions for hemorrhage control such as hemostatic wound dressings,8 14 20–22 tourniquets,9–13 15 16 18 19 24 and thoracotomy17 in the prehospital setting (military and civilian) were included (study participant n=35 666). Studies assessing tourniquets reported better hemodynamic control,10 with an improved shock index on arrival to the receiving facility (p=0.005).9 In addition, patients managed with tourniquets received fewer red cell and plasma units (p<0.001),9 though there was no associated survival benefit.10 19 Two studies reported a higher incidence of wound infections with tourniquet use.15 16 Four studies investigating the use of hemostatic dressings (HemCon (HemCon Medical Technologies, Portland, Oregon), QuikClot Combat Gauze (Z-Medica, Wallingford, Connecticut) or Celox (SAM Medical, Tualatin, Oregon)) demonstrated effective hemorrhage cessation and overall improved survival compared with non-hemostatic dressings.8 14 20 22
Airway management
Seven studies25–31 investigated different methods of prehospital intubation, such as supraglottic airway techniques (laryngeal mask airway (LMA), video laryngoscope (GlideScope), laryngoscope) and cricothyrotomy (n=9280). Overall, studies reported high success rates for all intubation methods. Studies evaluating prehospital endotracheal intubation reported that failed intubation varied between 0.7% and 31%.26 27 29 Expectedly, hospital mortality increased among those who could not be intubated en route.27 One study reported 80% successful placement and 10% mortality with LMAs after failed intubation,29 while another reported 82% success of cricothyrotomy as a rescue maneuver.31 Two other studies assessed airway management techniques such as supraglottic airway placement, bag mask ventilation and cricothyrotomy.25 28 Both studies reported no significant difference in adjusted survival comparing the different methods, though the studies were non-randomized and were methodologically and clinically heterogeneous.
Respiratory management
Twelve studies32–43 addressed respiratory management (n=2006), specifically needle decompression33 37–43 and tube thoracostomy.32 35 36 43 One study explored mechanical ventilation during patient transfer from a combat hospital to a medical center in Germany, assessing compliance of appropriate ventilator settings according to the ARDSNet (Acute Respiratory Distress Syndrome Network) guidelines. The study demonstrated an association between guideline compliance and decreased ventilator days, intensive care unit days, and 30-day mortality.34 Studies investigating needle decompression reported 76% failure (potentially correlated with chest wall thickness) with 39% performed in patients without pneumothorax.33 Overall, studies investigating prehospital thoracostomy reported a 5.2% to 27% increase in complications such as empyema, lung contusions, and pneumonia. Within these cohorts, patients with bilateral thoracostomies had increased incidence of pneumonia.32 35 36
Circulation
Eighteen studies were included44–61 (n=10 705), addressing civilian prehospital44 53 and combat45 51 58 transfusion, component therapy/factor VII (FVII),46 48–50 61 administration of tranexamic acid (TXA),55–57 59 use of temporary vascular shunts,54 methods of intraosseous access,60 and pelvic binder use.52 These studies assessing prehospital blood product transfusion compared with crystalloids reported no difference in survival, and increased overall transfusion requirements among those receiving prehospital transfusion.44 53 However, these patients had a better hemodynamic control, with higher blood pressure levels on emergency department (ED) arrival once adjusting for key factors.44 Conversely, a third study reported increased survival among those transfused in the prehospital combat setting compared with those with delayed or no transfusion.51 All patients had similar base deficit, pH and hemoglobin on ED arrival, although international normalized ratio (INR) and transfusion requirements were significantly different.51
Few studies assessed the use of prehospital allogeneic blood products or concentrate of clotting factors.44 45 51 53 Most studies were non-randomized and had methodological issues, which preclude definitive conclusions. No difference in mortality was identified in studies investigating component therapy compared with no component therapy or component therapy augmented with fresh whole blood (FWB), recombinant FVII, and whole blood.46–48 50 One study reported decreased odds of developing acute traumatic coagulopathy with use of component therapy augmented by FWB compared with component therapy alone.50 A recent RCT investigating the use of plasma compared with crystalloids in the civilian prehospital setting reported no differences in mortality, physiological variables, coagulation profiles, acute lung injury or multiple organ failure.61 In this study, short transport time and accessibility to plasma on arrival to the receiving facility may explain the negative outcomes. However, another similar prehospital multicenter RCT46 reported a lower 30-day mortality (p=0.03) associated with the use of thawed plasma versus usual care.
Studies assessing TXA administration reported no statistically significant mortality differences or safety concerns in relation to its use.55–57 59 However, the studies were mostly non-randomized and not powered to detect mortality.
One study investigated intraosseous access compared with intravenous access. The authors reported high success rates with intraosseous placement,60 and that intraosseous access accounted for ~12% of vascular accesses in their MEDEVAC population. One study assessed vascular shunt use in the prehospital setting in combat patients with lower extremity injuries. This study reported no difference in the amputation rate in the shunt group.54
Hypothermia prevention
Two studies describing interventions related to hypothermia prevention in prehospital civilian settings were included (n=68).62 63 One study evaluated the use of heating devices and intravenous tubing covers during air and land transport to warm intravenous fluids.62 The study analyzed rectal temperature on ED arrival in 12 patients with warmed intravenous fluids (36.8°C) and nine patients without (35.5°C). Another study compared passive warming (via polyester, wool and rescue blankets) with active warming (via chemical heat pad) reporting no significant differences in core body temperature between groups at any time points.64 However, both groups had statistically significant increase in temperature from transport to 30 minutes afterward.63
Mixed interventions
Two studies65 66 evaluated multiple interventions simultaneously, such as endotracheal intubation, cricothyrotomy, chest decompression, tourniquet use, etc (n=3925). The studies reported increased mortality among patients receiving life-saving interventions compared with those who did not.65 66 However, a matched propensity score analysis adjusting for injury severity, mechanism of injury, traumatic brain injury (TBI), and prehospital hemodynamics resulted in a statistically significant mortality reduction among the prehospital intervention group.66 One RCT assessed the use of long backboards versus vacuum mattress splints in 60 patients with possible spinal trauma in the civilian prehospital setting.67 The long backboard had quicker application and increased immobilization efficacy compared with the vacuum mattress splints.67
Extended focused assessment with sonography in trauma
Three studies assessed portable extended focused assessment with sonography in trauma (E-FAST) in prehospital settings68–70 (n=714). One study showed that E-FAST had comparable specificity to chest X-ray and was more sensitive for occult pneumothorax detection post-trauma.68 Another study reported high specificity, accuracy, and positive predictive and negative predictive values to detect free fluid in the chest/abdomen and hemothorax/pneumothorax.70 The authors concluded that E-FAST improves the ability to assess patients in austere air medical and prehospital environments, helps establish an early diagnosis, and decreases iatrogenic injury potential.
Risk of bias
Three RCTs46 61 63 had low risk of bias (tables 2–4, and online supplemental table 3). Forty-three (78%) of non-randomized cohort studies were classified as having poor evidence quality8 10–15 18–33 35 38 40–43 45 49 51 52 54 55 57–59 69 70 and 12 (22%)16 17 36 37 44 47 50 53 56 60 65 66 had good evidence quality as per the NOS. In addition, the diagnostic studies68–70 included in this review had a high overall risk of bias as per QUADAS-2.
Supplementary data
Newcastle-Ottawa case–control studies | appraisal results
Cochrane Effective Practice and Organization of Care risk of bias | randomized controlled trials
QUADAS risk of bias | diagnostic studies
Discussion
Main findings
The management of traumatically injured patients in combat settings has advanced considerably during the past two decades.71–73 The TCCC guidelines introduced standard practices focusing on point of injury/prehospital care, and en route care, therefore providing deployed healthcare workers with a framework to provide optimal care.74 In summary, the main findings of each of the MARCH components in the military and civilian prehospital settings were: (1) Massive hemorrhage: current evidence on tourniquets and hemostatic agents was of low quality. However, in the included studies, tourniquets provided bleeding control with consequent hemodynamic improvement. There is a paucity of high-quality clinical literature supporting the use of one type of hemostatic dressing over another in humans. (2) Airway: studies investigating various methods of airway management, such as laryngoscope, GlideScope, LMA, and cricothyrotomy, were also of low quality. Overall, these procedures had high success rates with better patient outcomes when performed en route to hospital. (3) Respiratory management: the evidence was also of low quality. Studies reported high failure rates of prehospital needle decompression. (4) Circulation: studies were of higher quality overall compared with the other MARCH domains and assessed prehospital blood products and TXA administration. However, studies assessing prehospital blood transfusion had conflicting results. Studies conducting adjusted analyses reported better outcomes with blood product transfusion compared with crystalloids. Non-randomized data assessing prehospital TXA use did not report improved outcomes. (5) Hypothermia prevention: studies had low methodological quality. However, all methods used to treat hypothermia were efficacious to maintain or increase body temperature measured on arrival to the receiving facility.
Knowledge gaps
Through evaluating current literature, an important knowledge gap was identified; while TCCC guidelines were developed to be applicable to all prehospital/combat environments, there is a paucity of MARCH intervention studies conducted in cold environments. This gap is significant, as it is vital to ensure that while working to minimize the effects of hypothermia for the casualty, it is equally important to ensure that any MARCH intervention remains effective in extreme cold conditions. The evidence focusing on hypothermia prevention is robust; however, very few studies investigating these interventions were conducted in the cold. Notably, the two studies investigating hypothermia prevention interventions identified through this review were of limited quality and were not conducted in a cold environment.62 63 These considerations raise important questions within each component of the MARCH interventions: (1) How do the physiological changes of hypothermia impact massive hemorrhage control? (2) Will below freezing temperatures impact respiratory interventions should the condensation freeze? (3) At what rates and temperatures do crystalloids and blood products freeze? Most countries with active military operations reach a wide range of temperatures; it is therefore vital for future research to investigate the efficacy of the MARCH interventions in colder environments, such that the TCCC guidelines can be expanded on to specifically combat the effects of cold environments, such as poor weather and icy conditions.75
We think that some of the evidence identified in the in-hospital setting may be transferable and adapted to the prehospital setting, such as the use of gum elastic bougie for endotracheal intubation. Few RCTs have been performed in ED and OR settings to evaluate the efficacy of bougies and stylets76–79; only one RCT compared the efficacy of an endotracheal tube introducer versus standard orotracheal intubation, reporting higher overall success rates and higher percentage of intubating difficult laryngeal views on first attempts in the endotracheal introducer group.80 One study assessed these techniques in the prehospital setting.81 Of these, a trial conducted in the ED reported significantly higher first-attempt intubation success using a tracheal tube introducer (bougie) versus an endotracheal tube with a stylet.76 In the prehospital setting, a recent retrospective review evaluated the variables associated with successful definitive airways in traumatically injured patients, and reported bougie use as one of the factors significantly associated with increased success rates.82 We think that these techniques are likely able to be adapted to prehospital settings, including austere and cold environments. However, future research is warranted.
In 2018, the finger thoracostomy (FT) was introduced to the TCCC guidelines as an additional treatment option for a suspected tension pneumothorax after two failed needle decompression attempts for combat casualties in refractory shock.83 One recent retrospective cohort study evaluated the efficacy of FTs in a helicopter emergency medical service (HEMS) setting, and reported a low complication rate in comparison to the needle decompression method.84 Additionally, in 2019, the iTClamp (Innovative Trauma Care, Edmonton, Alberta) was introduced in the TCCC guidelines in the management of craniomaxillofacial (CMF) injuries and penetrating neck injuries.85 The guidelines recommend the iTClamp be used as a primary treatment modality along with a TCCC-recommended hemostatic dressing and direct manual pressure. One case series investigating the efficacy of the iTClamp in the prehospital setting reported that 87.5% of cases (n=70) achieved adequate CMF hemorrhage control.86 Therefore, further research is warranted exploring the efficacy of these added interventions in all combat and austere environments.
In the military prehospital setting, blood transfusion has been widely studied leading to the adoption of blood product transfusion into civilian prehospital care.87 88 Through the literature identified in this review, studies assessing blood transfusion were of higher quality, though some reported conflicting results. Studies assessing mortality in this population are typically non-randomized and not powered to detect differences in meaningful clinical outcomes. However, it is reasonable to acknowledge the challenges associated with prehospital research in resuscitation of bleeding trauma patients, such as proper classification and enrollment of participants and proper randomization. Thus, blood product transfusion in the treatment of prehospital combat casualties and civilian trauma warrants continuing investigation in a variety of prehospital environments to generate robust evidence.89
Lastly, the safety and efficacy of TXA has been widely investigated in the perioperative environment and other clinical settings after the release of the Clinical Randomization of an Antifibrinolytic in Significant Hemorrhage (CRASH)-2 study.90 Overall, studies have demonstrated that TXA use is safe and is associated with both decreased requirements for allogeneic blood product transfusion and improvement of coagulation profiles.91 92 However, in prehospital environments, there is still room to improve evidence. The CRASH-3 study, a multicenter RCT conducted in patients with isolated TBI, assessed the use of TXA compared with placebo on hospital arrival.93 The study found no difference in TBI-related death, though identified increased efficacy with earlier treatment in those with mild to moderate TBI.93 Additionally, the risk of vascular occlusive events and seizures was similar between groups.93 A second study assessing patients with isolated brain injury given out-of-hospital TXA, the Resuscitation Outcomes Consortium (ROC) TXA trial, reported no difference in the neurofunctional outcome at 6 months after injury, in the 28-day mortality between groups, and in the progression of intracranial hemorrhage receiving TXA compared with the placebo group.94 Third, the recently published Study of Tranexamic Acid During Air Medical and Ground Prehospital Transport (STAAMP) trial, a further multicenter RCT conducted in prehospital trauma patients at risk of hemorrhage, reported no difference in 30-day mortality rates, 6 and 24-hour blood and blood component transfusion requirements, and in the incidence of pulmonary embolism or deep vein thrombosis in the group receiving prehospital TXA administration compared with placebo.95 However, in patients who received prehospital TXA administration within 1 hour of injury and in those with evidence of prehospital severe shock, post hoc subgroup analysis suggested that prehospital TXA is associated with lower 30-day mortality. Therefore, the CRASH-3 study, the ROC TXA trial, and the STAAMP trial have reported important differences and findings that warrant consideration and further investigation in studies with improved patient selection methods to further explore the efficacy of TXA in important clinical outcomes.
Strengths and limitations of this review
This is the first systematic review to appraise the TCCC literature and identify knowledge gaps on the management of trauma patients in civilian and military prehospital settings. In addition, the review highlights areas within these guidelines requiring further investigation. The primary limitation of this review is that most data identified are non-randomized, and therefore confounding is highly inevitable. As demonstrated through our findings, most advances relating to the MARCH components occur from registry-based quality improvement or observational cohort studies. Clinical and methodological heterogeneity between the study populations, interventions and measured outcomes introduces added difficulty in study comparability. However, research in trauma is challenging. Properly designed RCTs in prehospital settings are not always possible. In addition, funding for such studies is becoming increasingly difficult to obtain. Recent recommendations from the National Academies of Sciences, Engineering and Medicine are beginning to emphasize the utility of registry-based performance improvement as the optimal method of advancing care and outcomes in prehospital and military environments.96 In summary, though randomized evidence is lacking, it is equally important to acknowledge the complex reasons for which this deficit exists.
Future directions
We present preliminary recommendations and highlight areas notably requiring further investigation:
Expanding research on MARCH component interventions to include cold environments: While the MARCH interventions have been extensively investigated, several questions related to trauma patient management in cold environments remain unanswered. In 2020, the TCCC hypothermia protocol has been updated, along with the introduction of the Hypothermia Prevention Medical Kit80; however, there is a lack of any grade of evidence for the following subjects: (1) The speed at which crystalloids, blood products or other solutions may freeze in intravenous or intraosseous lines; and at what temperatures. (2) How to avoid this freezing process. (3) The effects of extreme low temperatures on tourniquet use. For example, does peripheral vasoconstriction from the cold warrant not using a tourniquet? (4) Will the warm ischemic time allowable be reduced such that peripheral amputations are more likely to occur? (5) Concerns surrounding the use of balloons (such as in resuscitative endovascular balloon occlusion of the aorta (REBOA)) in the cold environment. (6) Freezing of condensation within ventilator circuits. (7) The efficacy and safety of warming methods in the prevention and treatment of hypothermia specifically in cold environments, as these methods have been extensively investigated, though not specifically in cold settings.97–100
Transfusion of allogeneic blood products and use of clotting factor concentrates: Transfusion of red cells, plasma and platelets in a fixed ratio of 2:1:1 or 1:1:1 is currently well established within trauma literature, suggesting that hemostatic resuscitation should be initiated early for patients at risk of bleeding.101 While products like FWB can be refrigerated, the transport and use of allogenic blood products in prehospital environments still proves logistically difficult and requires further investigation. Recently, the interest in using FWB and cold stored whole blood in trauma resuscitation in prehospital settings has increased.102 Another promising blood component currently being investigated is freeze-dried plasma (FDP). FDP is plasma derived, lyophilized and can be reconstituted and administered rapidly for bleeding patients and patients with coagulopathy.103 Studies assessing feasibility and safety of FDP are under way.104 105 Furthermore, clotting factor concentrates such as prothrombin complex concentrate (PCC) and fibrinogen concentrate (FC) can be used in these settings as they are also lyophilized, easy to store, and can be reconstituted rapidly.106 107 The use of these products is promising, as they have easier transport logistics and are reported to be non-inferior or even superior compared with usual fixed plasma transfusion therapy or the use of cryoprecipitate to replace clotting factors and fibrinogen, respectively.108 A recent prospective study compared the use of FWB resuscitation versus blood component resuscitation in casualties treated in Afghanistan, and reported that, among critically injured patients, FWB transfusion was associated with improved survival compared with no-FWB, once stratifying by combat mortality index.109 Additionally, another recent retrospective matched cohort study compared trauma casualty coagulation profiles in a group treated with FDP versus without; this study reported a positive effect on coagulation profile, with no other significant effects in the FDP group versus the non-FDP group.110 We are conducting a multicenter RCT in Canada using FC and PCC on arrival to the trauma bay, compared with plasma, which will add important evidence on this subject.111 112 We recommend that early hemostatic resuscitation be used in patients at risk of bleeding and that further research be conducted addressing the use of FWB, FDP and clotting factor concentrates in various prehospital settings.
Mechanical hemorrhage control: Tourniquets for extremity injuries (Combat Application Tourniquet, Special Operations Forces Tactical Tourniquet) and hemostatic dressings (Combat Gauze or Celox/Celox Rapid gauze) are recommended for mechanical hemorrhage control as described above. For junctional areas (neck, axilla, and groin), junctional tourniquets might be useful (Combat Ready Clamp, SAM Junctional Tourniquet, Junctional Emergency Treatment Tool) and the XSTAT device (which injects absorbent sponges into deep wounds) can be applied to tamponade bleeding.113–115 However, data on these devices are scarce, and mostly conducted in manikins and healthy volunteers.116–118 In addition to the above, research is necessary to evaluate the efficacy and safety of the more recently implemented iTClamp in prehospital and austere environments.
TXA in the prehospital setting: Future trials addressing TXA in the prehospital setting should focus on improving patient selection and testing different TXA regimens in severely injured patients. As demonstrated in the ROC TXA trial,94 the use of 2 g of TXA given as bolus is safe. This regimen may be more feasible in the prehospital setting, including in distant austere and cold environments.
REBOA: REBOA has emerged as a technique for truncal hemorrhage control and may improve non-compressible truncal hemorrhage mortality. The evidence on REBOA use in hospital is evolving. However, there is little evidence on the safety and efficacy of its use in the prehospital setting including austere and cold environments. Currently, REBOA is appropriate for surgical teams in combat settings, and teams with immediate surgical capability.119–125 Few studies have reported that REBOA improved hemodynamic status of hemorrhaging patients in military settings, with increased survival rates, though a higher percentage of failure126–128 and distal thrombosis123 129 is also reported. Continued research is strongly recommended to better understand its role in prehospital and austere settings.2
Conclusions
This review summarizes the main aspects of the evidence focusing on diagnosis and treatment, and the use of techniques and devices in the prehospital civilian or military settings. The difficulties in conducting RCTs in these settings are recognized. Future studies should further address interventions, techniques and devices pertaining to the MARCH criteria in the military and civilian environments. More specifically, more robust evidence addressing existent or new interventions, techniques, and devices in cold environments is important to develop the foundation of care for trauma patients in these environments.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Footnotes
RS and IM contributed equally.
Contributors LTdL, RS, IM, and LP conceived and designed the study. RS, IM, and LP led the production of the review across the different phases, supervised by LTdL, who is the methodology expert and senior author. RS, IM, and LP led the entire screening process, data retrieving, and analyses as per the PRISMA protocol, with the other authors (EB, HP, WS-K, HT, AN, AB, and JC). These processes were monitored by LTdL. HT, AB, JC, and AN were the content experts and contributed significantly to the article review. RS and IM along with the assistance of LP drafted the article and were supervised by LTdL. All authors contributed to the revision of the article. All authors have seen and approved the final article version. RS and IM take responsibility for the article as a whole.
Funding This article was performed for Task 47 under a research contract W7714-145967 with the Defence Research and Development Canada (DRDC).
Competing interests JC received research support from Canadian Blood Services and Octapharma.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}