

Abstract
Background Delirium has been shown to prolong the length of intensive care unit stay, hospitalization, and duration of ventilatory control, in addition to increasing the use of sedatives and increasing the medical costs. Although there have been a number of reports referring to risk factors for the development of delirium, no model has been developed to predict delirium in trauma patients at the time of admission. This study aimed to create a scoring system that predicts delirium in trauma patients.
Methods In this single-center, retrospective, observational study, trauma patients aged 18 years and older requiring hospitalization more than 48 hours were included and divided into the development and validation cohorts. Univariate analysis was performed in the development cohort to identify factors significantly associated with prediction of delirium. The final scoring system for predicting delirium was developed using multivariate analysis and internal validation was performed.
Results Of the 308 patients in the development cohort, 91 developed delirium. Clinical Frailty Score, fibrin/fibrinogen degradation products, low body mass index, lactate level, and Glasgow Coma Scale score were independently associated with the development of delirium. We developed a scoring system using these factors and calculated the delirium predictive score, which had an area under the curve of 0.85. In the validation cohort, 46 of 206 patients developed delirium. The area under the curve for the validation cohort was 0.86, and the calibration plot analysis revealed the scoring system was well calibrated in the validation cohort.
Discussion This scoring system for predicting delirium in trauma patients consists of only five risk factors. Delirium prediction at the time of admission may be useful in clinical practice.
Level of evidence Prognostic and epidemiological, level III.
Introduction
Delirium is an acute disorder of consciousness characterized by a variable course of cognitive decline. Previous reports have indicated that its incidence in the intensive care unit (ICU) is high, ranging from 20% to 80% depending on the study population and method of diagnosis.1–3 Delirium has been shown to prolong the length of ICU stay, hospitalization, and duration of ventilatory control, in addition to increasing the use of sedatives and increasing the medical costs.3–5
Delirium can be assessed in ICU patients through several tools, including the Confusion Assessment Method-ICU (CAM-ICU), which has the highest sensitivity and specificity.6 7 This tool is crucial for rapid treatment of delirium.8 9 Moreover, risk factor prevention has been shown to reduce both the incidence and the duration of delirium.10 11 The 2018 Pain, Agitation, Delirium, Immobility, and Sleep guidelines listed the risk factors for the development of delirium, which included history of dementia, hypertension, alcoholism, presence of severe disorder of consciousness, and critical illness at admission, as well as use of benzodiazepines.12
There is a need to predict delirium, and to date several scoring systems have been proposed. The PRE-DELIRIC (PREdiction of DELIRium in ICu patients) model is based on factors available within 24 hours of ICU admission.13 In addition, another scoring system was developed that included six factors.14 Although many studies have been conducted on delirium prediction in patients entering the ICU for internal medicine and postoperative care, few have been conducted on trauma patients. These patients and those with traumatic brain injury (TBI) are often excluded from studies on delirium due to data collection and interpretation difficulties.15 However, it is important to include these patients as traumatic injuries can occur in all individuals irrespective of age.
This study aimed to develop a scoring system for predicting delirium in trauma patients, based on factors available at the time of admission, to prevent its incidence and manage these cases appropriately.
Patients and methods
Study design, setting, and participants
This single-center, retrospective, observational study was performed at the emergency and critical care center of Saga University Hospital. Patients aged 18 years and older who were admitted to our emergency center with traumatic injuries between April 1, 2015 and March 31, 2019 and requiring hospitalization equivalent to ICU or high-care unit for more than 48 hours were included in this study (N=664). Patients who had been treated at other medical institutions and were then transferred to our hospital (n=15), those whose consciousness did not improve and were unable to communicate verbally with the medical staff or family members until the time of discharge (n=38), pregnant women (n=2), and patients who were unable to communicate in Japanese (n=4) were excluded from this study. Patients, family members, and guardians who declined participation were also excluded, as were those with incomplete medical records at admission (n=45). We also excluded patients who were alcoholics (n=26). We defined an alcoholic as a patient who drinks heavily on a daily basis and for whom a clinician judges that prevention of alcohol withdrawal delirium is necessary. Finally, we excluded patients who were admitted to the hospital while abusing narcotics or stimulants (n=0).
A total of 514 cases were analyzed in this study (figure 1). All eligible patients provided informed consent with the opportunity to opt out.
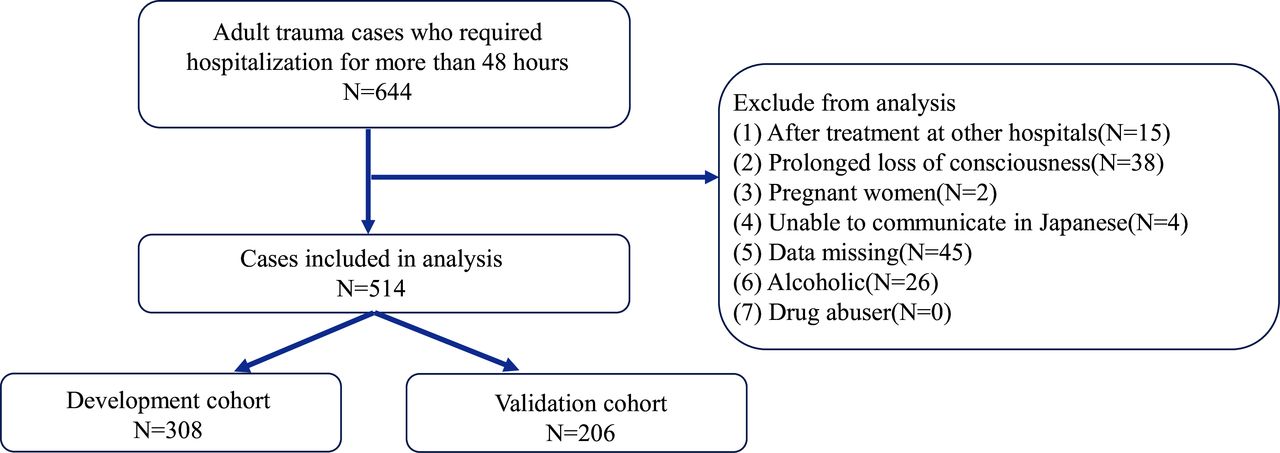
Patient selection flow chart. A total of 664 cases met the inclusion criteria and 514 cases were included in the analysis after exclusion (59.9% in the development cohort and 40.1% in the validation cohort).
Diagnosis of delirium and data collection
The presence of delirium was assessed by analyzing the medical records and calculating the CAM-ICU. The characteristics assessed in this scoring method included acute changes or fluctuations in mental status, inattention, disorganized thinking, and altered level of consciousness. Delirium was identified as the presence of the first two criteria, and either the third or fourth.16
Collected data included age, sex, body mass index (BMI; weight (kg)/height2 (m2)), Clinical Frailty Score,17 18 Charlson index,19 smoking, alcohol consumption, and dementia history. The Clinical Frailty Score is described in table 1. We also extracted vital signs at the time of admission (blood pressure, heart rate, body temperature). Further details such as Glasgow Coma Scale (GCS) score, Revised Trauma Score (RTS),20 Injury Severity Score (ISS),21 presence of TBI, and laboratory data such as fibrinogen, fibrin/fibrinogen degradation products (FDP), hemoglobin, C-reactive protein (CRP), and lactate levels were extracted.
Clinical Frailty Score
Statistical analysis and model development
The entire cohort was randomly divided into two, the development cohort (n=308, 59.9%) and the validation cohort (n=206, 40.1%). The assignment was done by generating random numbers, sorting them in ascending order, and dividing them into the top 60% and the bottom 40%. The development cohort was divided into two groups based on the presence or absence of delirium. Factors significantly associated with development of delirium were analyzed using Wilcoxon’s test for continuous variables and χ2 test for categorical ones. P<0.05 was used to denote statistical significance. A stepwise method was used to select variables for the prediction equation among those significantly associated with onset of delirium. Variables that were found to be correlated by the Spearman’s rank correlation test were excluded and logistic analysis was performed. The performance of the final scoring system was expressed in terms of discrimination and calibration. The former was calculated by the area under the receiver operating characteristic (ROC) curve.22 Youden’s index was used to determine the optimal cut-off, and the sensitivity and specificity were calculated. The latter was assessed by the Hosmer-Lemeshow goodness-of-fit test and calibration plot. All statistical analyses were performed using the JMP Pro V.14 software package (SAS, Cary NC, USA) and R V.4.1.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Model development
The development cohort consisted of 308 patients, 91 of whom developed delirium. The univariate analysis revealed that age, sex, low BMI, Clinical Frailty Score, Charlson index, history of occasional drinking, history of smoking, presence of dementia, GCS score, heart rate, body temperature, hemoglobin level, FDP, lactate level, CRP, RTS, ISS, and presence of TBI were significantly associated with the development of delirium (p<0.05) (table 2). Of these variables, the predictors chosen for the final scoring system based on the multivariate analysis were GCS score, BMI, Clinical Frailty Score, FDP, and lactate level. The following equation was derived:
Baseline characteristics and univariate analysis of the development and validation cohorts
Delirium predictive score (DPS)=−0.4670−(0.2218×GCS)−(0.09790×BMI)+(1.131×Clinical Frailty Score)+(0.002645×FDP)+(0.3196×lactate level).
Therefore, the probability of developing delirium (PDD) was given by the following equation:
PDD=1/(1+exp(−DPS))
The PDD value ranges from 0 to 1, which indicates the probability of developing delirium.
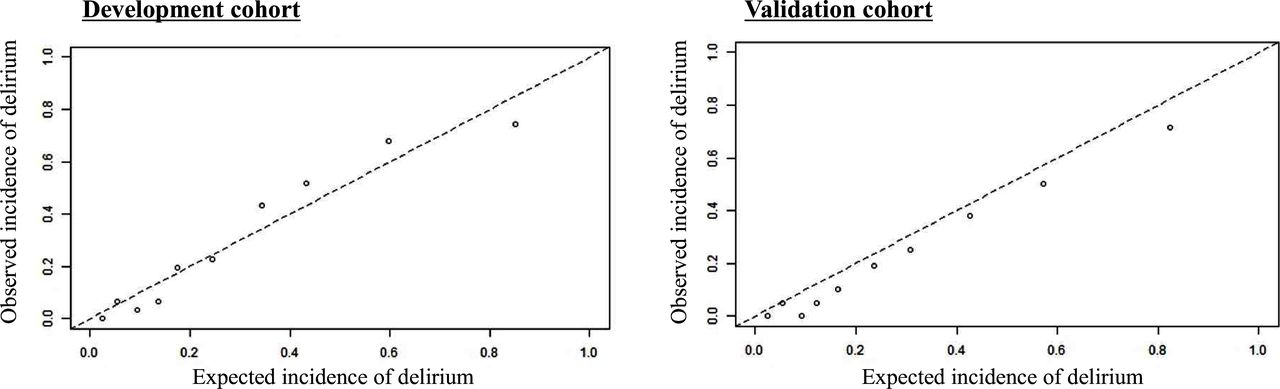
Youden’s index was used to determine the optimal cut-off, and the results showed that a DPS of −0.72 had the highest sensitivity and specificity at 78.0% and 82.0%, respectively. The negative predictive value was 89.9%, and the positive and negative likelihood ratios were 4.33 and 0.27, respectively. The area under the ROC curve (AUC) was 0.85 (95% CI 0.80 to 0.89) (figure 2). As shown in the calibration plot analysis, DPS appeared to be well calibrated in the development cohort (figure 3).

Delirium predictive score receiver operating characteristic curve in the development and validation cohorts. The area under the curve (AUC) was 0.85 (95% CI 0.80 to 0.89) in the development cohort and 0.86 (95% CI 0.79 to 0.91) in the validation cohort.

Calibration plot of the delirium predictive score in the development and validation cohorts. The horizontal axis shows the expected incidence and the vertical axis shows the actual measured incidence of delirium.
Internal validation
The validation cohort consisted of 206 patients, 46 of whom developed delirium. DPS was applied to the validation cohort and ROC analysis was performed, resulting in an AUC of 0.86 (95% CI 0.79 to 0.91), with 91.3% sensitivity and 67.5% specificity (figure 2). The Hosmer-Lemeshow goodness-of-fit test demonstrated no significant evidence for the DPS (p=0.32). As shown in the calibration plot analysis, DPS appeared to be well calibrated in the validation cohort as well (figure 3).
We divided the validation cohort into several subgroups for further analysis. In the group with TBI (n=51), the AUC was 0.76 (95% CI 0.61 to 0.87), and in the group without TBI (n=155) the AUC was 0.89 (95% CI 0.80 to 0.94). In the group with occasional drinking (n=99), the AUC was 0.83 (95% CI 0.72 to 0.90), and in the group without occasional drinking (n=107) the AUC was 0.88 (95% CI 0.78 to 0.94).
Discussion
The scoring system we developed consisted of patient characteristics in terms of clinical frailty and BMI, and trauma severity in terms of GCS score, FDP, and lactate level. It has generally been reported that older age is a risk factor for the development of delirium, as is Clinical Frailty Score,23 and in this study the latter was the most significant contributing factor. We speculate that the Clinical Frailty Score, which reflects age, activities of daily living, and health, is crucial in describing patient characteristics. In this study, age and Clinical Frailty Score were found to be strongly associated as per the Spearman’s rank correlation test. Because age is reflected in the Clinical Frailty Score, we excluded it from the factors of the delirium prediction model in the development cohort.
In the development cohort, the delirium group had a significantly lower BMI than the group without delirium. Although the details regarding this association are unknown, it has been previously reported that low nutritional status during hospitalization is associated with an increased risk of developing delirium, and it is possible that the BMI at the time of admission reflected the nutritional status prior to injury.24
TBI has been shown to be a risk factor for delirium.15 Since it is associated with hypercoagulation and hyperfibrinolysis from the early period after injury, FDP and D-dimer levels are likely to be elevated.25 26 FDP is a useful biochemical marker for assessing severity and mortality in patients with blunt trauma, with or without head injury.27 28 In this study, we think that FDP reflected the presence of head trauma or trauma severity in patients without head injuries.
Elevated lactate levels are observed not only in patients with shock due to severe trauma but also in those with multiple trauma and relatively stable hemodynamics.29 They are also elevated in patients with other diseases that cause hypoxemia, which has been reported to be a risk factor for the development of delirium.30 Lactate levels, also strongly related to the onset of delirium, are likely to play an important role in our scoring system. All of the factors included in this system have been previously shown to be associated with the development of delirium. However, there have been no previous reports on developing such a system for trauma patients using these factors and this study is the first to do so. The relationship between trauma and delirium has been studied in elderly populations and among those with high illness severity, which is very limited.15 23 Our study included younger patients, as well as less severely injured ones, who are generally considered less likely to develop delirium.
In the subgroup analysis, patients with TBI are considered to be at higher risk of developing delirium, and this prediction model can be applied to this patient group. Patients with TBI are more likely to have low GCS score and coagulation-fibrinolysis system abnormalities. We think that the inclusion of GCS score and FDP as components of the present prediction model enabled us to predict delirium in patients with TBI.
Assessing the risk of developing delirium at admission may lead to more careful observation of the patients and less oversight of insomnia symptoms and restlessness. Identifying a delirium high-risk group may also enable us to identify the group of patients who would benefit from early preventive intervention for delirium. We would like to collect more data on the changes in delirium prevention and management by applying this prediction model.
This study has several limitations. First, it is generally thought that environmental factors also play an important role in the development of delirium,31 which were not assessed in this study. Second, this was a single-center study and similar results may not be obtained at other facilities. Third, there are some significant issues due to the retrospective design. The onset of delirium was identified by CAM-ICU assessment based on the medical record entries by physicians and nurses. Thus, the timing of charting was not always uniform, and the number of charts per day varied depending on the patient and severity of illness. Furthermore, the patients were not observed by medical staff trained in delirium assessment. The subtypes of delirium can be divided into hyperactive, hypoactive, and mixed motor subtypes,32 and some reports suggest that the hypoactive subtype is difficult to diagnose, which may have been overlooked and underestimated.33 In addition, this was a retrospective study and it was difficult to identify the subtype of delirium. Therefore, we think that future prospective studies are needed to determine whether this prediction model is applicable to all delirium subtypes. The CAM-ICU evaluation of patients with impaired consciousness due to TBI may be difficult and lead to diagnostic errors and biases. Alcoholism and drug abuse may be significant contributors to the development of delirium. In this study, only 26 of the trauma patients were alcoholics and none were narcotics or stimulant abusers. Therefore, we are yet to test whether the delirium prediction model developed in this study can be applied to these populations. In this study, we excluded patients who were clearly suspected of alcoholism and who required prevention of alcohol withdrawal delirium. However, since we could not obtain accurate information on the history of alcohol consumption from the patients’ medical records, we cannot deny the possibility that some of the patients diagnosed with delirium using the CAM-ICU included patients with alcohol withdrawal delirium. To overcome the limitations mentioned above, prospective multicenter validation studies should be conducted in the future.
Conclusion
In this study, we established a new scoring system that predicts delirium in trauma patients and included BMI, lactate levels, Clinical Frailty Score, FDP, and GCS score as variables. This system provides a more accurate method of predicting delirium. Future studies are needed to validate these results.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethics committee of Saga University Hospital (approval no: 2021-02-R-05).
Footnotes
Contributors AMa, TM: conceptualization, methodology, formal analysis, investigation, writing - original draft. MM, TG, AS, HY, MKom, MH, KM, KS, KN, RS, MA, AF, KY, SN, MKob: formal analysis, investigation. HK: formal analysis, investigation, writing - original draft. AK: methodology, formal analysis, investigation, writing - original draft. THM, YS: conceptualization, methodology, writing - original draft, guarantor. AMo: conceptualization, methodology, formal analysis, investigation, writing - original draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}