

Case presentation
An adult male patient in his 30s, with no medical history was admitted to a local hospital after sustaining a fall off an 8 m high scaffold. Initial clinical assessment revealed an unconscious patient with a GCS of 8/15 (eye opening: 1; verbal response: 2; motor response: 5), pupils equal and reactive to light, a pulse of 107 bpm, a blood pressure of 100/60 mm Hg, a respiration rate of 24cpm, with an O2 saturation of 87% on ambient air. The patient was intubated and a full-body CT scan was performed revealing a 4 mm frontoparietal subdural hematoma, an undisplaced fracture of the right frontal bone with a subgaleal hematoma and an ipsilateral eyelid edema, a right hemopneumothorax along with pulmonary contusion and ipsilateral flail chest as well as a subcutaneous emphysema spreading to the neck. No injuries were found in the abdomen. An X-ray of the upper right limb revealed a fractured humerus stabilized using a brace.
The hemopneumothorax was drained but the patient developed shortly afterwards a hypotension of 80/50 mm Hg refractory to volume expansion using isotonic saline. A femoral central venous line was taken and norepinephrine was initiated. A FAST (Focused Assessment with Sonography for Trauma) examination was performed and came back normal. The patient was referred to Mohammed VI University hospital for specialized management.
The patient was admitted within an hour and a half from the causing accident. At admission, our assessment found an unconscious patient, intubated and ventilated, anisocoric, with a blood pressure of 95/50 mm Hg under norepinephrine, a heartbeat of 120 bpm, a respiration rate of 26 cpm and a O2 saturation of 95% under mechanical ventilation. A continuous infusion of norepinephrine was maintained through a subclavicular central venous line, and blood pressure was invasively monitored using an arterial line.
We performed a full-body enhanced CT scan revealing the same head injuries as the initial CT along with a subarachnoid hemorrhaging and a cerebral edema without a mass effect. In the thorax, it revealed a bilateral pneumothorax more prominent on the left, a right hemothorax, a pulmonary contusion in the superior left lobe as well as the lower right lobe with multiple pneumatocele, a reduced caliber of the mediastinal great vessels, and a chest tube placed in the left pleural cavity (figure 1). Abdominal images revealed a Grade 1 liver trauma in the fifth and sixth segments, a Grade II right renal trauma, and a peritoneal effusion. The bone window revealed fractures through the lateral curvatures of ribs 3 to 12 on the right.

Axial lung window images showing a bilateral pneumothorax more prominent on the left, pulmonary contusion with multiple pneumatocele, a chest tube placed in the left pleural cavity.
Laboratory tests revealed a hemoglobin at 6,4 g/dL, a 19% hematocrit, a platelet count of 138 000, fibrinogen levels at 0,8 g/L, a 46% prothrombin ratio, an aPTT (activated partial thromboplastin time) of 1.02 s, HS Troponin levels at 1932 ng/L. The patient’s blood type was O positive, and we transfused 3 units of packed red blood cells, 2 units of Fresh Frozen Plasma (FFP), and 5 units of platelet concentrate.
There was no emergency surgical procedure needed at the time being (in concertation with the surgical team).
Given the sustained hemodynamic shock in spite of volume expansion and the use of norepinephrine, and in light of the high suspicion of myocardial contusion (given the blunt chest trauma, the nature of the chest injuries, and the sustained hemodynamic instability along with high troponin levels), we decided to initiated continuous dobutamine infusion as well.
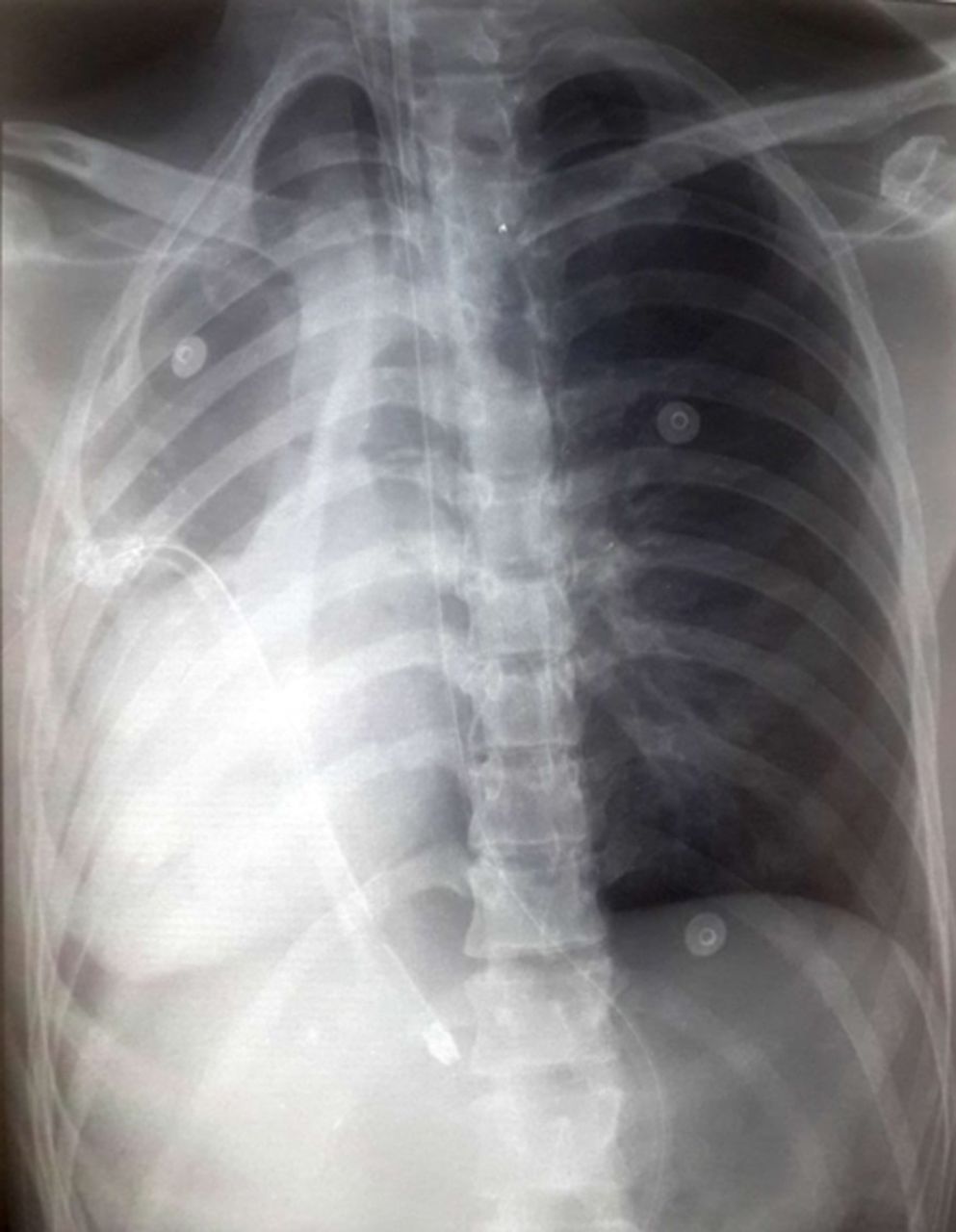
A follow-up physical examination revealed deviated heart sounds to the right, subsequently an in-bed plain Chest X-ray (CXR) was performed revealing a right sided heart (figure 2), confirmed by a transthoracic echocardiography (TTE).

Plain chest X-ray showing a right sided heart.
What would you do?
Maintain vasopressors and perform another chest CT
Skip CT and perform a mini-invasive exploratory operation (video-assisted thoracoscopic surgery (VATS)
Skip CT and rush the patient for an exploratory open chest operation
What we did and why?
We opted for an immediate exploratory thoracotomy which unveiled a large tear in the right lateral pericardium with a cardiac herniation into the right chest aggravated by a left hemothorax, as well as torsion of the great vessels (figure 3). The hemothorax was drained by opening the left pleura, the heart was manually reintroduced within the pericardial cavity thus reducing the torsion of the great vessels, the pericardial tear was sutured, and a chest tube was placed in the left pleural cavity.
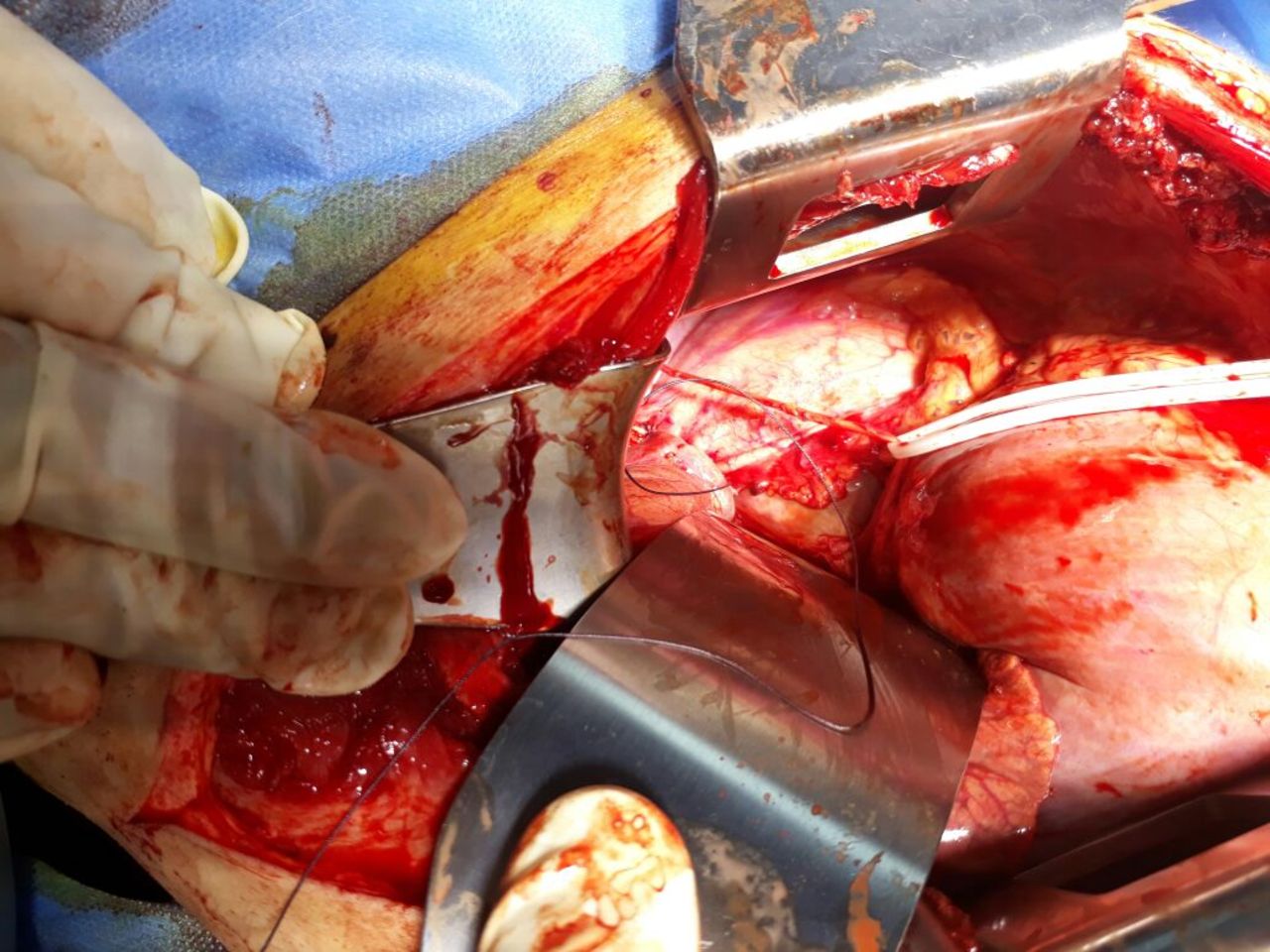
Preoperative image showing a ruptured pericardium with an exteriorization of the heart rotated rightward without rupture of the large mediastinal vessels.
Postoperative assessment unveiled a blood pressure of 120/70 mm Hg and a heartbeat of 95 bpm. Follow-up laboratory tests revealed a hemoglobin at 11.9 g/dL, a 36% hematocrit, a 54% prothrombin ratio, and an aPTT of 1.38 s. Follow-up TTE was normal.
The patient was kept under mannitol and sodium valproate, sedated by midazolam and ketamine, and curarized using atracurium. We used Sufentanil for analgesia. Cerebral blood flow was monitored daily using transcranial Doppler. As for thromboprophylaxis, we used compression stockings during the first 72 hours before introducing enoxaparin 40 mg/day subcutaneously in concertation with the neurosurgical team.
The patient was later on weaned off drugs and extubated, undergoing daily sessions of physical therapy before he was discharged within 4 weeks after initial admission.
Pericardial rupture is a rare complication of blunt chest trauma, a subsequent cardiac herniation with dextrocardia through the pericardial tear is even a rarer and often fatal condition.1
A right-sided herniation (as is the case for our patient) may result in a torsion of the large vessels causing a decrease in venous return and cardiac output, leading to a cardiogenic shock and subsequent cardiovascular instability.2
Thoracic imaging remains the main diagnostical tool. In-bed chest XR and echocardiography are very useful in unstable patients hospitalized in intensive care unit although of limited value in the case of a left cardiac luxation. Chest-CT—if and when the patient’s condition allows—remains the gold-standard imaging.
Another challenge is delayed herniation of the heart through the pericardial rupture. In fact, Graef et al3 reported that secondary heart herniation accounted for 34.7% of cases and are arguably attributed to vibration and shearing forces caused by abnormal movements, which is undoubtedly what happened to our patient who was moved multiple times, explaining why initial radiological assessment showed no cardiac herniation.
The treatment is surgical, the approach is often based on an ipsilateral thoracotomy, although cases of sternotomy, clamshell thoracotomy and VATS were reported.3 The heart is reinserted into the pericardial cavity, and the pericardial tear is closed using sutures or a patch-plastic. In cases of myocardial strangulation an extension of the pericardial tear may be required.3
In terms of prognosis, no recent literature data are available as only scattered cases were reported. Older literature data reported a survival rate of 33% up to 40%.1 The outcome relies mainly on the diagnostical delay and associated injuries in poly-trauma patients.
In polytrauma patients, such an injury is associated with a high mortality due the delay in diagnosis, especially in cases of delayed herniation and/or the associated extrathoracic injuries at the forefront of a polytrauma clinical picture.
In our case, although prior imaging did not show a herniated heart (even though a pericardial tear could not be excluded) and the hemodynamic instability could be explained otherwise, our team still prompted the question of a potential heart injury, which was diagnosed and managed promptly with a favorable outcome.
Ethics statements
Patient consent for publication
Footnotes
SB and MZB are joint first authors.
Contributors S.Berrichi: co-first author, patient management, paper conception, data collection, writing, and editing. M.Z.Bouayed: co-first author, article conception, data collection, writing, and editing. S.Amaqdouf: contributor; A.Abetti: contributor; S.Berrajaa: contributor. I.Benaini: contributor. H.Bkiyar, N.Ismaili, N.ElOuafi, B.Housni: supervision, data and article review, and validation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}