

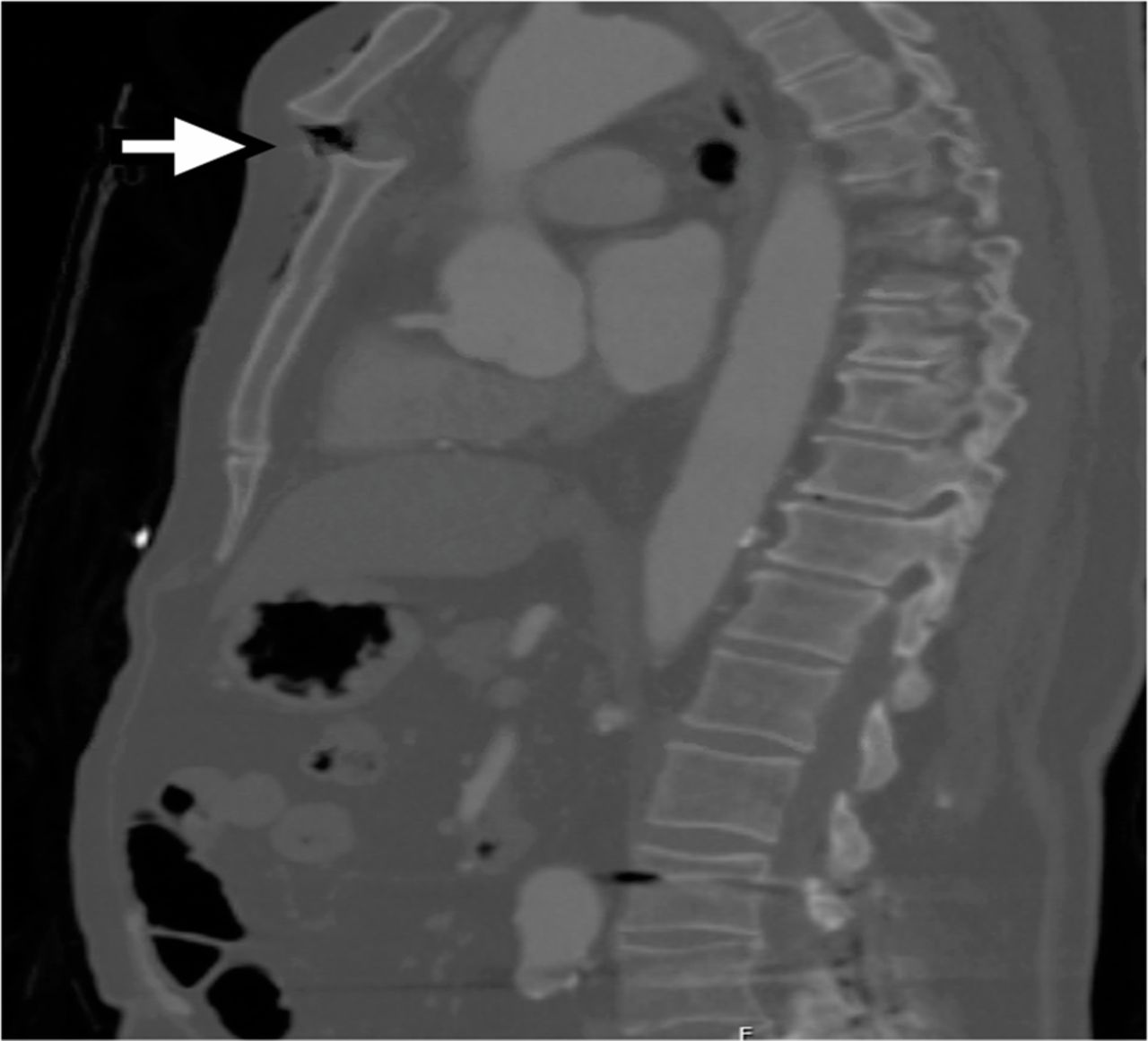
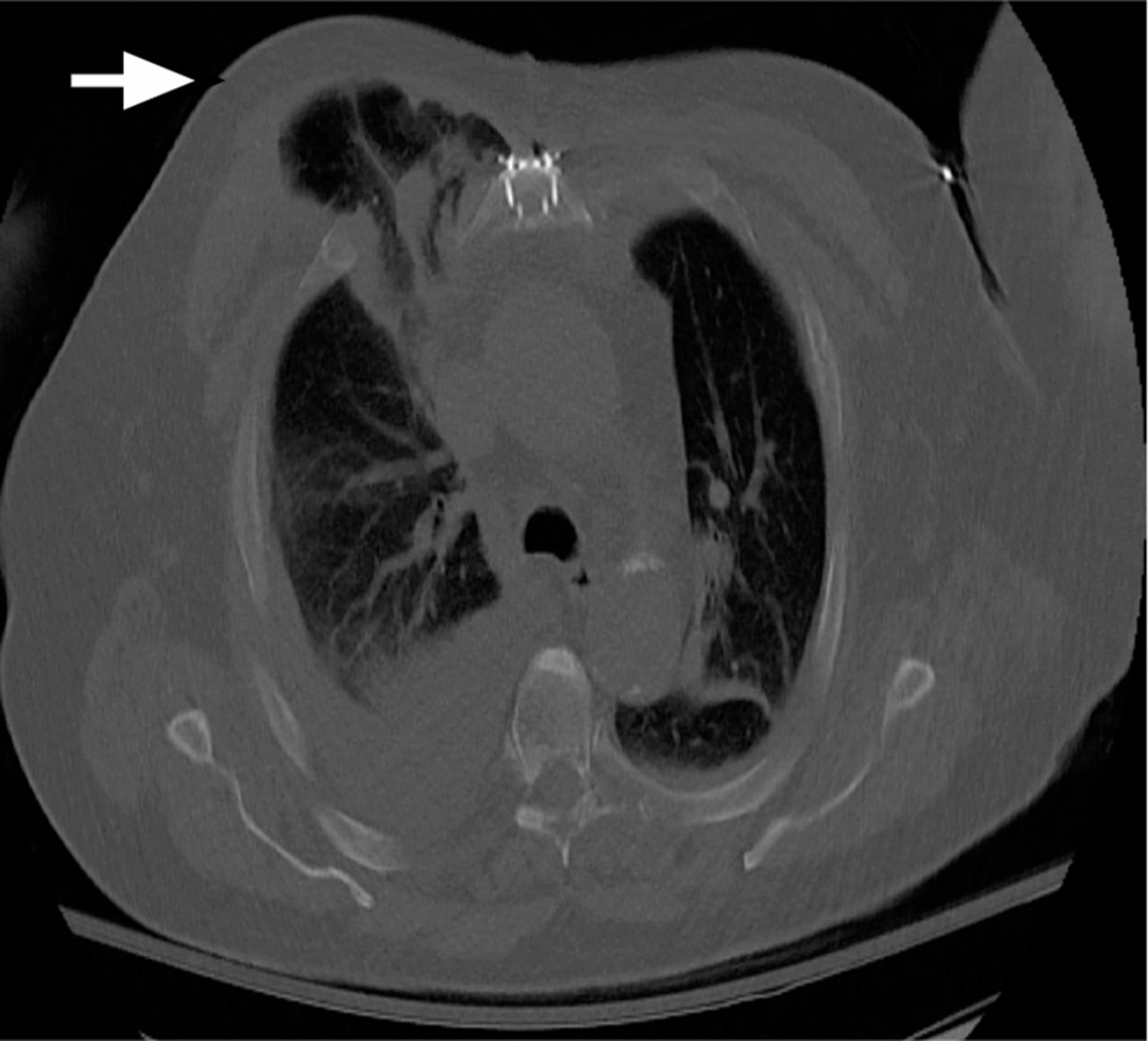
A male patient in his 70s presented after a farming tractor ran over his chest. On arrival to the trauma bay he was hemodynamically stable, with significant chest pain and paradoxical movement of his chest with respirations. Cross-sectional imaging revealed a sternal fracture, moderate posterior displacement of the sternomanubrial joint, left-sided second through fourth rib fractures with moderately sized hemothorax and a right sixth rib fracture (figure 1). A left-sided chest tube was placed. The patient was taken to the operating room on hospital day 2 for reduction of the sternomanubrial dislocation and open reduction with internal fixation (ORIF) of the sternum by plastic surgery. He was successfully extubated on postoperative day 1. On postoperative day 5, the patient was noted to have a prominent bulge on his right anterior chest, most pronounced during inspiration. CT of the chest revealed herniation of portions of the right upper and middle lobe through the right anterior chest wall, with right second and third costosternal dislocations and fractures of the adjacent third through fifth costal cartilage (figure 2). A large pleural effusion was also noted. Shortly after, the patient developed respiratory failure requiring intubation.

Sagittal CT showing sternomanubrial dislocation (arrow).

Axial CT showing lung herniation through the costochondral fractures (arrow) after sternal ORIF.
What would you do?
Observation with potential plans for elective repair.
Reduction of lung hernia and stabilization of costal cartilage fractures with metal plates.
Reduction of lung hernia, mesh placement and stabilization of costal cartilage fractures with resorbable plates.
Reduction of lung hernia, mesh placement and removal of sternal hardware.
What we did and why?
Answer C.
A pigtail catheter was first placed which evacuated over a liter of fluid from the left chest. Due to the patient’s acute respiratory failure, the decision was made to proceed with surgical intervention with a multidisciplinary approach that included thoracic surgery and trauma.
We began by reopening the previous sternal incision to evaluate the area of the sternum lateral to the sternal ladder plate. The sternal ladder plate appeared to adequately reduce and align a significantly injured sternum. No room lateral to the plate was present for us to secure hardware.
Lung herniation was evident though a major disruption of the right second and third costal cartilages. Meticulous dissection allowed for reduction of most of the herniated lung. An infraclavicular counter incision was required to fully reduce the lung. With the lung fully reduced, additional fractures of the fourth and fifth costal cartilages were visualized. With the sternal plate in place, there was no margin laterally on the sternum to secure hardware. In view of the significant injury to the sternum and the adequacy of the current sternal plate, the decision was made to place a Vicryl mesh in underlay fashion and stabilize the fractured cartilages using resorbable stabilization plates (BioBridge, Acute Innovations, Hillsboro, OR). We elected to use Vicryl mesh due to evidence of a small air leak intraoperatively and the subsequent concern for infection of a permanent mesh and the resultant potential for sternal hardware infection. Each plate was secured laterally to the rib and medially to the sternum using Ethibond (Ethicon, Somerville, New Jersey, USA) suture cerclage with puncture of the rib using a cutting needle (figure 3). The patient tolerated the procedure well, was extubated on postoperative day 1 and was discharged to a subacute rehabilitation facility by postoperative day 8.
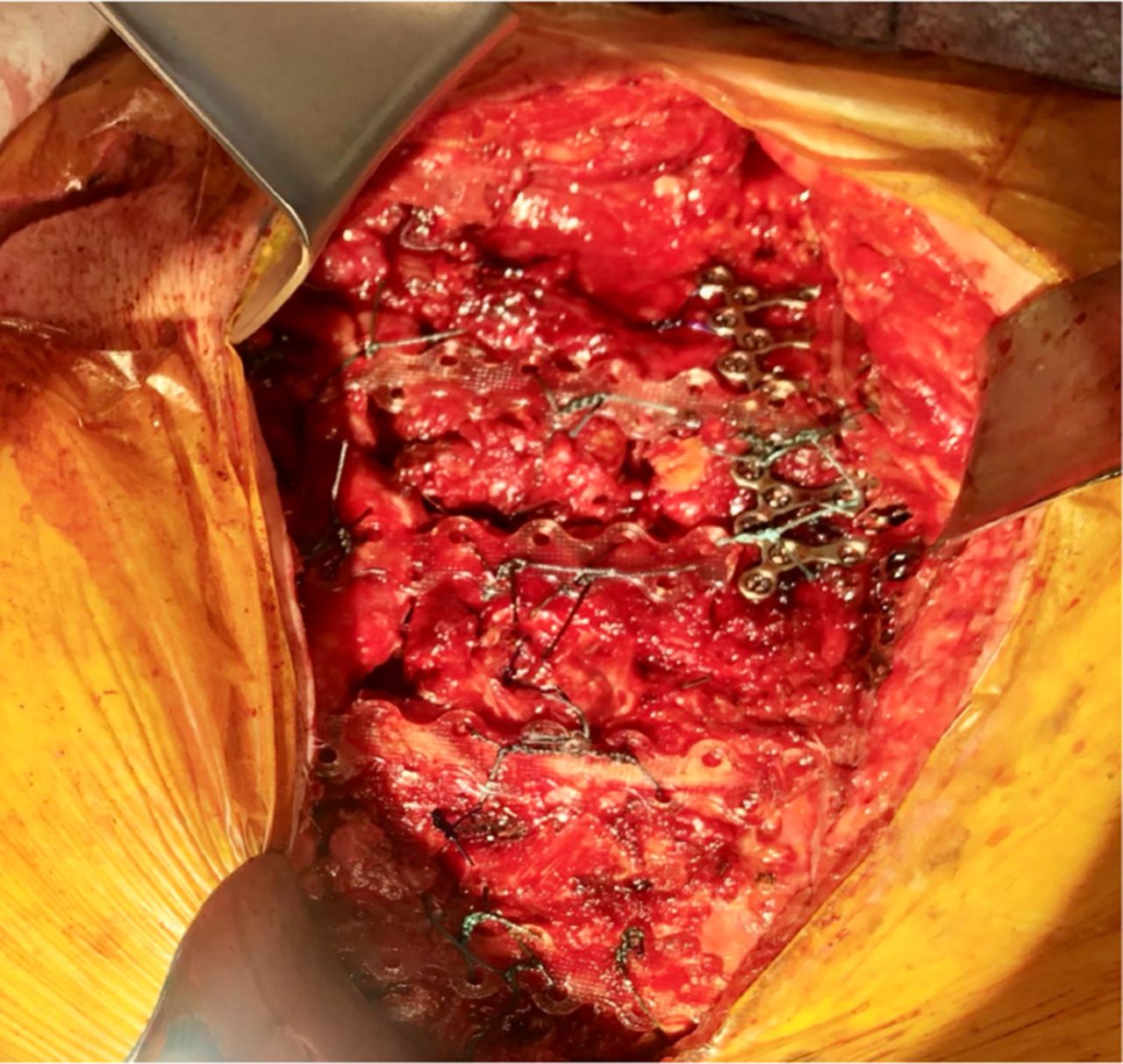
Intraoperative image after completion of repair of the costochondral cartilage fractures using resorbable plates with suture cerclage technique.
Traumatic lung herniations remain a rare clinical entity, especially through defects in costal cartilage. Although surgical stabilization of rib fractures has gained popularity, management of costal cartilage fractures remains controversial. A literature review of the limited reports available suggests that other operative options for traumatic lung herniations include spanning the cartilage with hardware from the ipsilateral rib to the sternum or contralateral rib, sternal wire repair or use of polytetrafluoroethylene mesh. To date, no study has compared the long-term outcomes of these operative approaches.
Ethics statements
Patient consent for publication
Footnotes
Contributors SP and DR contributed to article creation and revision. DW, JG and MK contributed to article revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}