

History
A 41-year-old man was shot in the proximal left groin with a handgun of unknown size. The emergency medical service noted exsanguinating hemorrhage with dark venous blood and applied a dressing under manual pressure.
Examination
The patient was confused and agitated and had a blood pressure of 70/50 mm Hg, heart rate of 130 beats per minute, and a respiratory rate of 25 breaths per minute. He was intubated rapidly, intravenous catheters were inserted into the upper extremities, and more dressings were applied to the area of bleeding in the left groin.
Question
Appropriate management of this patient in the emergency center would be:
Apply a tourniquet directly to the entrance wound.
Obtain vascular control in the trauma room.
Fill the entrance hole of the missile with hemostatic gauze.
Transfer the patient to the operating room.
Management
After the patient’s skin was prepared and draped from the umbilicus and both lower extremities circumferentially to the toenails, a 10 cm longitudinal incision was made over the left femoral vessels. Torrential venous hemorrhage was noted from both large and small veins as two attending surgeons used large metal clips, 2-0 silk ties, and DeBakey vascular clamps to attain hemostasis. After transfusion of 42 units of packed red blood cells and an unknown number of units of fresh frozen plasma and platelet packs, reasonable control of venous hemorrhage was noted. Examination of the left groin first documented that there were no injuries to the left common femoral, superficial femoral, and profunda femoris arteries. In contrast, two-thirds of the left common femoral vein, the femoral vein in the groin, and the profunda femoris vein were destroyed.
Question
With the venous injuries in the left groin as described, the appropriate management would be:
Ligate the ends of the common femoral and femoral veins.
Insert an 18 Fr thoracostomy tube as an intraluminal shunt.
Insert an externally supported 12 mm polytetrafluoroethylene (PTFE) graft.
Create a spiral vein graft from the right greater saphenous vein.
Management
With the patient’s hypothermia and acidosis correcting under anesthesia once hemorrhage had been controlled, it was noted that there was continued venous oozing from all surfaces in the left groin incision. This was thought to be due to obstruction of all venous return from the left lower extremity, except through the left greater saphenous vein. After a brief discussion regarding the merits of inserting a temporary venous intraluminal shunt versus definitive reconstruction of venous outflow, the two attending surgeons agreed to perform the reconstruction.
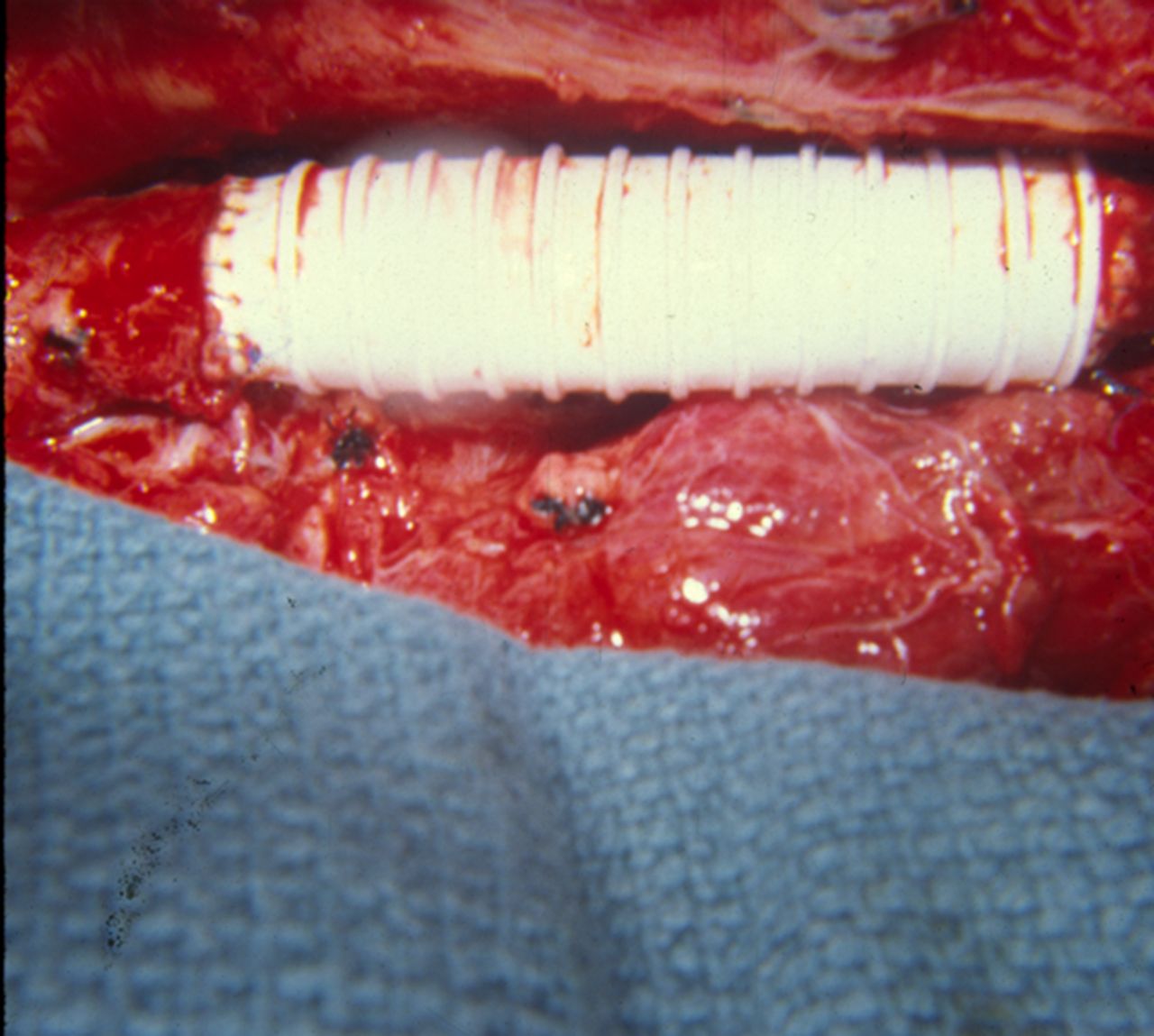
A 12 mm ringed PTFE interposition graft was inserted from the left femoral vein inferiorly to the remnant of the left common femoral vein inferior to the inguinal ligament (figure 1). Both end-to-end anastomoses were performed with 5-0 polypropylene sutures; flushing both ends of the proximal anastomosis before completion did not demonstrate any thrombus and the suture lines were hemostatic. It was noted that the venous oozing in the left groin incision ceased immediately.
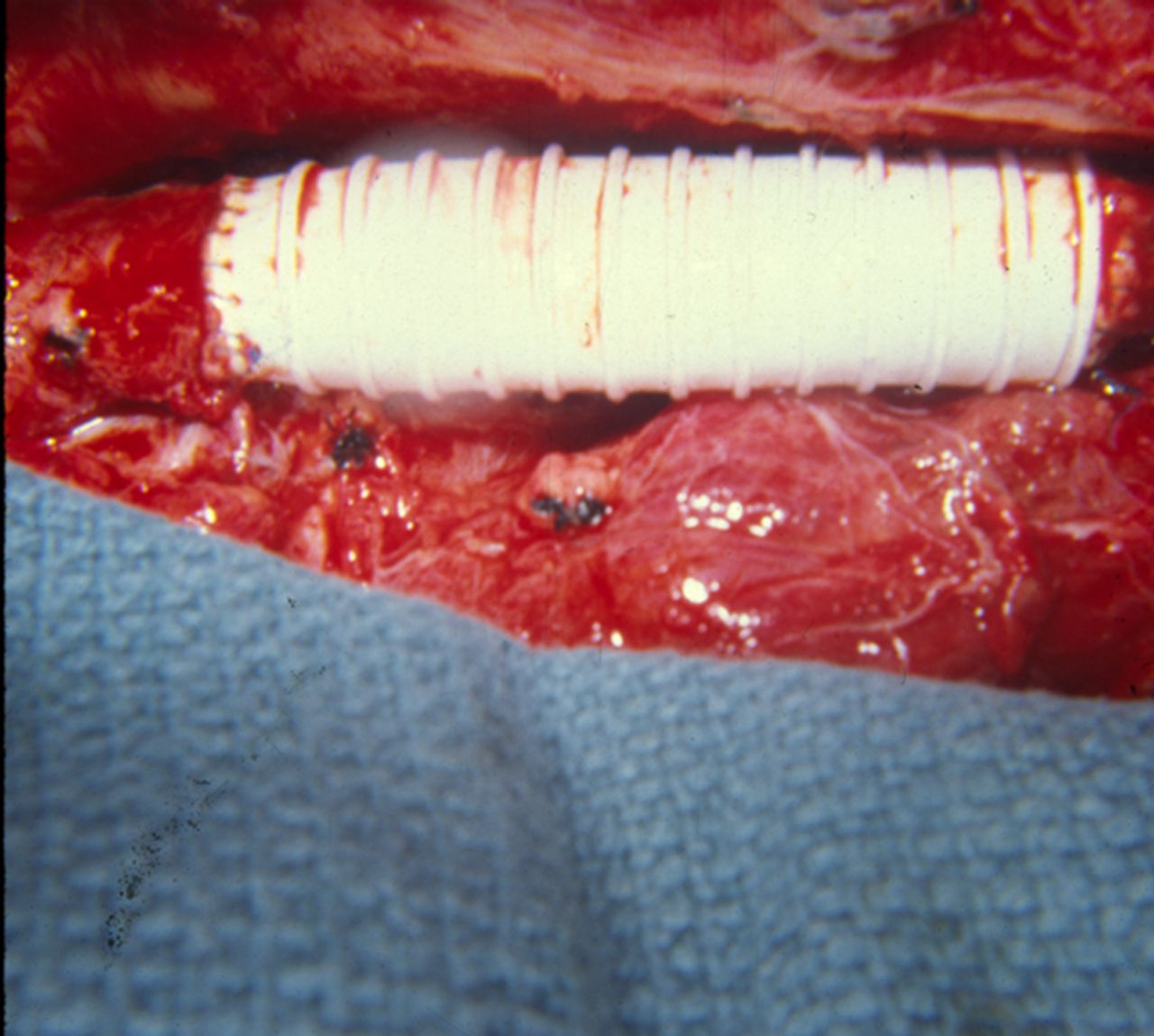
A 12 mm ringed polytetrafluoroethylene graft from the left femoral vein to the common femoral vein after gunshot wound to the groin.
After irrigation with a saline-antibiotic solution, the left groin incision was closed in layers. Pressures in the left below-knee musculofascial compartments were 18 mm Hg in the anterior compartment and 15 mm Hg in the deep posterior compartment and so fasciotomy was not indicated.
In the intensive care unit, the left lower extremity was wrapped with a compression bandage and elevated on one pillow. Oral aspirin 81 mg tablets were administered every 12 hours. The patient was kept on bed rest for 4 days, and only trace edema of the left ankle and foot was noted. He was then allowed to walk with crutches while the entire left lower extremity had compression wraps applied.
The patient was discharged on the 12th day after injury using crutches and compression wraps when walking, 81 mg oral aspirin each day, and with strict admonitions to avoid prolonged sitting or flexion of the left knee and smoking.
When seen in the postoperative clinic 3 months after injury, his left groin incision was healed and there was 1+ edema of the left ankle and foot. His oral aspirin tablets were discontinued, and the strict admonitions listed above were re-emphasized to the patient.
Discussion
The management of complex peripheral venous injuries has been discussed in several vascular case reports.1–4 This is a reflection of the significant frequency of such injuries in trauma centers with 20% to 30% penetrating wounds, the 200-year uneven history of attempts at venous repair, and the persistent lack of concern about performing ligation rather than repair.5 6
Reasons to perform repair of injured major veins (common femoral, femoral, popliteal/tibioperoneal) of the lower extremities were first described during the Korean War and then expanded during the Vietnam War and beyond7–9 (Box 1). Data on the short-term and long-term patency during the last two decades confirm the value of attempts at venous repair.10–13
Reasons to perform repair of injured major veins of the lower extremities
Prevent early decrease in arterial inflow, particularly if there are simultaneous injuries to the artery and vein.
Decrease venous pressure to control oozing from soft tissue and fasciotomy incisions.
Decrease acute and chronic edema in the distal lower extremity.
Even if gradual thrombosis of the venous repair occurs, this allows time for venous collaterals to dilate.
Short-term and long-term patency of properly performed venous repairs is good to excellent.
Options for repair of an injury to a major vein of the lower extremity are listed in Box 2. Of these, patch venoplasty (sizing difficult to assess, extensive suture material involved), panel vein graft (tedious to construct, extensive suture material involved, limited patency), and spiral vein graft (same as panel vein graft) are used rarely in the modern era.
Options for repair of a venous injury in the lower extremity
Lateral venorrhaphy.
Segmental resection with end-to-end anastomosis.
Segmental resection with interposition graft.
Contralateral non-reversed saphenous vein graft.
Ringed polytetrafluoroethylene graft.
Patch venoplasty.
Panel vein graft: two vein segments are bivalved, connected posteriorly, and sutured together anteriorly, usually over a stent.14
Spiral vein graft: a long segment of vein (see the following formula) is bivalved, wrapped around a cylinder of appropriate size, and sutured to form a large length of autogenous tube14: composition formula: length of donor vessel=radius of recipient vessel/radius of donor vessel × length of recipient vessel.
When a complex venous reconstruction is performed, thrombus should be flushed or irrigated out of the proximal and distal vein before and just prior to completion of the last anastomosis. If a venous PTFE interposition graft is to be inserted, the largest appropriate size is chosen as a narrow graft in a non-pulsatile system will likely thrombose in the postoperative period. End-to-end anastomoses do not require the traditional three-point or two-point fixation sutures (Carrel-Guthrie) as the lumen is usually larger than the adjacent artery; however, these may be necessary with anastomoses in the popliteal or tibioperoneal vein behind or inferior to the knee joint. In the low pressure venous system, any type of venous repair can be performed with 5-0 or 6-0 polypropylene suture. Finally, with prolonged clamping to complete a complex venous repair, it is worthwhile, if the surgeon is a “believer,” to check ipsilateral below-knee compartment pressures before taking down the drapes.
There is no consensus on postoperative management after complex venous repairs. Significant elevation of the ipsilateral leg and foot lowers arteriolar inflow and, with swelling of soft tissue and ligation of venous collaterals during surgery, can theoretically increase the risk of a below-knee compartment syndrome. The two components of management that have always made sense to the author are early administration of aspirin and compression wraps to “drive” venous return through the repair in the deep (major) veins, especially during walking.
Conclusion
When dealing with a major venous injury in the lower extremity in a non-damage control situation, repair should always be considered.
Ethics statements
Patient consent for publication
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}