Article Text

Summary
A 90-year-old man was transferred to a geriatric evaluation and management (GEM) unit for management of hypoactive delirium following a pneumonia and acute myocardial infarction complicated by septic shock. He was found to have central hypothyroidism and hypoadrenalism leading to the diagnosis of hypopituitarism. Cerebral imaging confirmed this was secondary to a pituitary haemorrhage. This case illustrates the complexity of assessment of delirium and its aetiologies. Hypoactive forms of delirium in particular can be difficult to detect and therefore remain undiagnosed. While this patient's delirium was likely multifactorial, his hypopituitary state explained much of his hypoactivity. His drowsiness, bradycardia, hypotension and electrolyte imbalance provided clinical clues to the diagnosis.
Statistics from Altmetric.com
Background
The state of delirium has been described for hundreds of years and is said to derive from the Latin word ‘delirare’ (‘to be out of one's mind’).1 It occurs in 11–42% of general medical inpatients.2
The cardinal manifestations are cognitive disturbance with impaired orientation, temporal fluctuation and onset over a few hours or days. Three clinical subtypes of delirium have been described based on arousal disturbance and psychomotor behaviour. These include a hyperactive/hyperaroused or agitated subtype, a hypoactive/hypoaroused or lethargic subtype and a mixed subtype with alternating features of the hyper and hypoactive forms.3
Hypoactive delirium, which is also associated with a poorer prognosis, is probably more common than the hyperactive type but is frequently missed. This contributes significantly to the 30 to 60% of all cases of delirium that remain undiagnosed.4 ,5 Therefore, hypoactive delirium poses a special diagnostic problem because the patient's attention deficit may seem to reflect nothing more than impaired cognitive performance. Failure to make an early diagnosis can result in delayed investigations and specific treatment.6
As a disease with non-specific symptoms, which is relatively uncommon and under-investigated in the elderly, hypopituitarism can be easily overlooked as a cause of delirium. Nevertheless, a proper diagnosis and therapy are of the utmost importance, as the clinical consequences of untreated disease can be severe.7–9 In older people, the finding of biochemical central hypothyroidism can often be the first clue.10
Case presentation
A 90-year-old Caucasian man was transferred to a geriatric evaluation and management (GEM) unit after admission to a tertiary hospital in Melbourne, Australia. His initial presentation was with septic shock in the setting of a left lower lobe pneumonia. This was complicated by acute renal impairment, acute myocardial infarction and delirium. Vasopressor support in the intensive care unit was required.
His medical history included hypertension, hypercholesterolaemia and excised squamous cell carcinoma of the skin. Prior to this presentation, he lived with his wife in his own home, functioning independently and mobilising with a four-wheeled frame. He was a vegan with no history of cigarette smoking and no alcohol consumption. He was not known to have any family history of significance.
His medications on admission were pantoprazole, dalteparin, ramipril, bisoprolol, aspirin, simvastatin, hypromellose—dextran 70 eye drops, metoclopramide and lactulose.
On admission to the GEM unit, he was still confused in the setting of resolving delirium and was unable to recall the sequence of events during his admission to hospital. Most history was obtained through medical records and collateral information from his wife.
Initial physical examination revealed a frail, elderly man who was drowsy but easily rousable. Orientation to person was intact but not to time or place. Of note, his lying blood pressure was reduced at 90/53 mm Hg and he was bradycardic with a heart rate of 53 bpm and regular. Respiratory rate was 18 breaths/min and oxygen saturation was normal on room air. Tympanic temperature was 36.5o celsius. Assessment of fluid status indicated euvolaemia. Cardiovascular examination revealed only an aortic sclerotic murmur. Bilateral coarse crackles of the middle and lower zones of the lungs and a generalised expiratory wheeze were audible on auscultation. Abdominal examination was unremarkable and neurological examination, limited by participation, did not reveal significant abnormalities. In particular, there was no obvious visual field defect.
Triceps reflexes were normal; others could not be elicited.
Investigations
Laboratory investigations (summarised in table 1) revealed a normochromic, normocytic anaemia with mild thrombocytosis. Leucocytes were 7.7 with normal differentiation. Hyponatraemia (sodium 131 mmol/L) and hyperkalaemia (potassium 5.4 mmol/L) were present. His urea was 8.2 mmol/L, creatinine was 144 umol/L and estimated-glomerular filtration rate (eGFR) was 40 mL/min (which was the worst eGFR during his entire admission). His C reactive protein was 41.
Biochemical and hormonal lab results prior to and after treatment of hypopituitarism
Thyroid function was checked as part of a routine delirium work-up, especially given his bradycardia. These levels were consistent with central hypothyroidism with thyroid-stimulating hormone (TSH) 0.05 mIU/L (normal range 0.27–4.20), free T3 3.5 pmol/L (normal range 3.9–6.7) and free T4 of 7.1 pmol/L (normal range 12–22). This finding, added to his electrolyte profile and haemodynamic status suggestive of hypoadrenalism, raised suspicion of hypopituitarism and a complete set of relevant endocrinological blood tests confirmed the diagnosis.
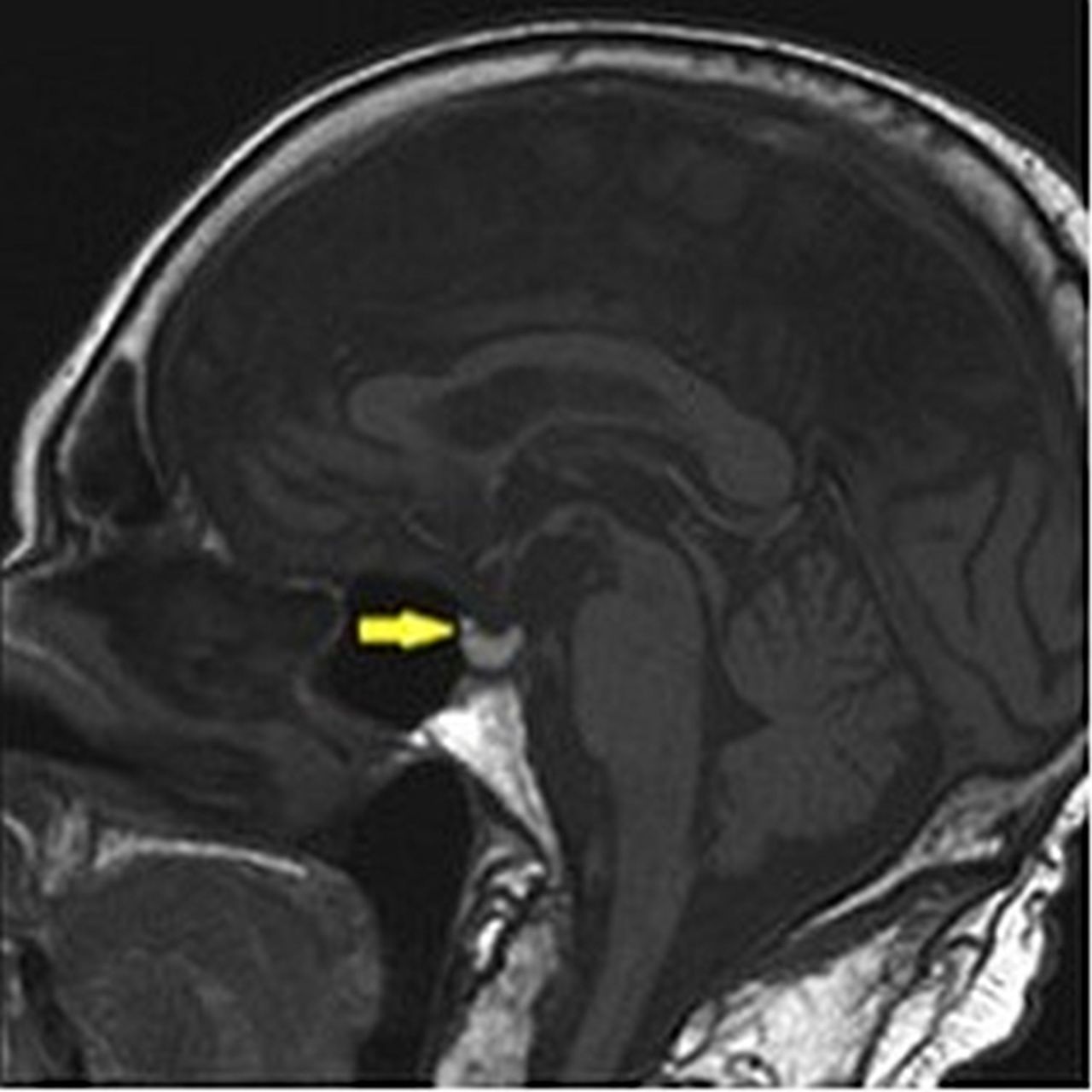
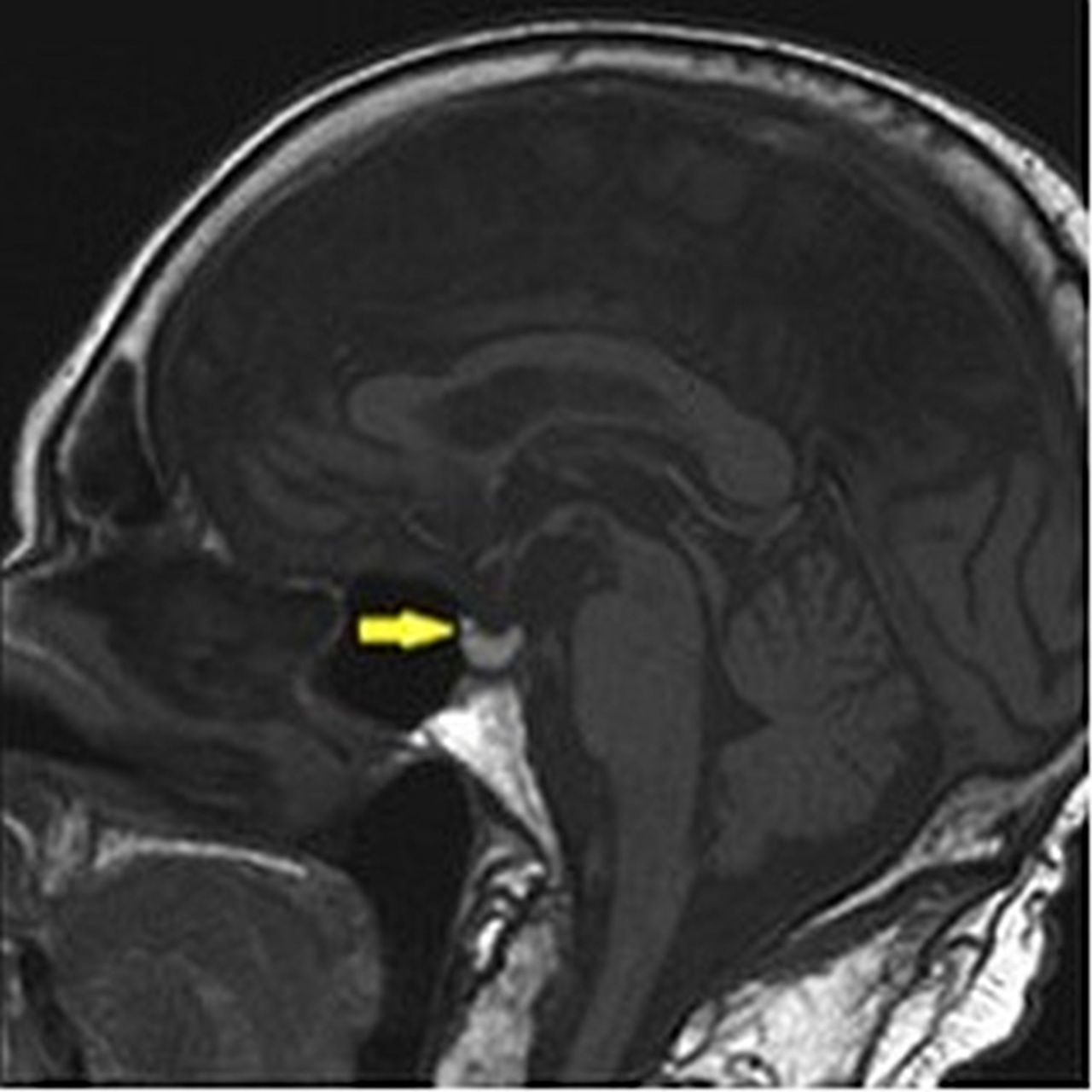
Brain MRI revealed acute pituitary haemorrhage and age-appropriate, global cerebral atrophy. No other intracranial pathology was identified (figure 1). The posterior pituitary was intact.
{kind=link}
Pituitary MRI—pituitary apoplexy (yellow arrow).
Treatment
Specialist endocrinological advice was sought and steroid and thyroid hormone replacement therapy was started. This included initial intravenous hydrocortisone (dose and for how long), switching to oral cortisone acetate (25 mg at 8:00, 10 mg at 18:00) on the sixth day and oral thyroxine (50 μg daily). Testosterone replacement was considered unnecessary in the acute stage. Other supportive treatment for delirium was continued.
The neurosurgery team were contacted and they advised for conservative treatment.
Outcome and follow-up
A significant haemodynamic improvement was evident within 24 h following start of the above treatment, and the patient's conscious state also gradually improved. A return to premorbid level of mobility and independence was achieved over the next fortnight.
Hormonal investigations were repeated at about 4 months (table 1) and an endocrinologist reviewed the patient at that time. Education was provided to the patient and his wife regarding sick day management of steroid replacement and he was referred back to his local doctor for on-going monitoring.
Discussion
Delirium is a multifactorial disorder. Factors that increase the risk for delirium can be categorised into those that increase baseline vulnerability and those that precipitate the disturbance. Underlying brain diseases including dementia, stroke, Parkinson's disease, advanced age and sensory impairment are among the predisposing factors whereas polypharmacy, infection, dehydration, immobility, malnutrition and the use of bladder catheters are categorised as precipitating factors.
A change in the level of consciousness is often the first clue. When delirium is suspected the Mini-Mental State Examination (MMSE) or other simple bedside tests of attention must be performed. Where the patient appears awake enough, the ability to focus, sustain or shift attention can be assessed during attempts to obtain a history. Excluding a progressing dementia causing the cognitive impairment requires knowledge of the patient’s baseline level of functioning and can be quite challenging.
Hypoactive delirium is associated with lethargy in its mildest form. These patients can be easily overlooked on a busy ward, since they may respond appropriately, if monosyllabically, to greetings and brief questions. If they are noticed to be unusually listless, this may be attributed to depression or to lack of motivation.11 Patients with a more marked form of this variant may be very withdrawn and almost mute and may tend to drift off to sleep in the middle of conversation. In its most extreme form, it merges into stupor from which the patient can be aroused only by vigorous and repeated stimuli.12
Delirium should be initially diagnosed from its clinical manifestations. A number of instruments are also available for this purpose; a popular one is the Confusion Assessment Method ‘CAM’ (Box 1),13 which is a suitable tool for use in critically ill patients.14 This diagnostic tool has 94% to 100% sensitivity and 90% to 95% specificity.
The Confusion Assessment Method (CAM) diagnostic tool
-
CAM diagnostic tool
-
Acute onset and fluctuation
-
Inattention
-
Disordered thought
-
Altered conscious state
-
-
Diagnosis requires presence of the first two criteria and either of the second two.
To investigate the underlying cause, a comprehensive physical examination is imperative where possible. Drug toxicity accounts for approximately 30% of all cases of delirium.15 Thus, the most important initial step is a medication review taking into account all over-the-counter agents and drugs belonging to other household members.
Series of investigations including laboratory testing (serum electrolytes, creatinine, glucose, calcium, complete blood count, urinalysis and culture, drug levels and toxic screening) and neuroimaging are recommended to investigate the underlying cause of delirium. The latter is particularly recommended when the cause of delirium is not apparent from the initial evaluation.
Hypoadrenalism directly16–18 and indirectly through hyponatraemia19 ,20 could contribute to the development of delirium and delusional ideas. Common medical disorders and surgical interventions cause increased cortisol demand, which in patients with subclinical hypoadrenalism, may precipitate adrenal crisis21 (Addisonian crisis). Although it can be treated easily, hypoadrenalism is notoriously difficult to diagnose as it can mimic many other illnesses.
The association of hypothyroidism with clinical and biochemical evidence of hypoadrenalism raised the possibility of pituitary insufficiency in our patient. Another clue is the finding of normochromic normocytic anaemia, which is reported in 20% of elderly patients with hypopituitarism.22 A peculiar issue in the primary presenting features of hypopituitarism in the elderly is hyponatraemia, which in this particular population is usually ascribed to intercurrent illness or drugs (eg, diuretics). Older patients are particularly prone to this hydroelectrolytic complication, which can cause neurological symptoms such as headache, nausea, disorientation and lethargy, and culminating in coma.23
Hypopituitarism is an often neglected and subtle condition, which in the elderly is frequently under-diagnosed because it is not suspected and, therefore, investigated. Many correlated symptoms overlap with those that can be seen as part of the normal ageing process. The delayed diagnosis and therapy can lead to serious systemic complications. As far as is known, only one population-based study has evaluated the prevalence (45.5 cases per 100 000) and incidence (4.2 cases per 100 000) of hypopituitarism in the adult population (mean age at diagnosis: 50 years; range 18–79 years).24 No gender differences were noted.
The most frequent causes of hypopituitarism are pituitary and extra-pituitary tumours, pituitary surgery, cranial irradiation, infiltrative disorders and pituitary apoplexy. The latter diagnosis is an acute, rare but life-threatening haemorrhage or infarction of the pituitary, in which an underlying pituitary adenoma is usually present. Death may follow with acute pituitary insufficiency due to pituitary ischaemia or haemorrhagic infarction. The typical symptoms are headache, nausea, vomiting, visual disturbance, altered mental status and panhypopituitarism.25–27
The clinical manifestations of hypopituitarism are diverse and variable, depending on the extent and duration of pituitary hormone deficits. In addition to the signs and symptoms of specific hormone deficits, patients often present with symptoms and signs related to the cause of hypopituitarism, including symptoms related to mass effects or clinical manifestations related to and caused by excessive hormone secretion.28
Corticotropin and thyrotropin deficiencies result in fatigue, weakness and slowed mentation. Gonadotropin and growth hormone deficiencies, although less critical in the acute phase of illness, have the potential to lessen patients’ quality of life in the longer term.
The diagnosis of hypopituitarism is made by documenting subnormal secretion of pituitary hormones in defined circumstances. Each pituitary hormone axis must be tested separately. The diagnosis requires the measurement of basal and stimulated secretion of anterior pituitary hormones and their target hormones. Hypothyroidism in patients who have a pituitary or hypothalamic disease is the result of TSH deficiency. Therefore, unlike in patients who have primary thyroid disease, an elevated serum TSH concentration cannot be used to make the diagnosis. The serum TSH concentration is usually not low either, unless the hypothyroidism is treated. Screening for hypothyroidism in patients with pituitary or hypothalamic disease is therefore performed by measuring thyrotropin level as well as total or free thyroxin level.
Clinical and/or biochemical evidence of hypopituitarism calls for imaging of the hypothalamopituitary region and MRI is currently the first choice modality.
The treatment of delirium should be directed to the causes of delirium, its manifestations or both. Symptomatic treatment can be either with drugs or through non-pharmacological means. Non-pharmacological strategies predominantly focus on supportive care of the delirious patient and include keeping the patient in a quiet and safe environment, enlisting the patient's family members for the purposes of reassurance and reorientation, providing an optimal level of stimulation with fixed day/night rhythm, promotion of mobility and implementing relaxing music and smells.29
In our patient, pharmacotherapy was directed at the underlying cause, which was found to be hypopituitarism. As for primary hypothyroidism, Levothyroxine is the treatment of choice in central hypothyroidism, but must be preceded by proper adrenal replacement therapy. The starting dose must be low and gradually increased over time in order to avoid subclinical/clinical hyperthyroidism. Therapy with androgens in the elderly is indicated only in symptomatic hypogonadal patients without evidence of absolute contraindications (such as prostate or breast cancer). Thorough examination of red blood cell count, haematocrit and lipid profile is also recommended prior to treatment initiation.
Detailed discussion on diagnosis and treatment of panhypopituitarism is out of the scope of this case report.
Learning points
-
Delirium is a multifactorial disorder that can be precipitated by any medical condition in a susceptible person, therefore a comprehensive history and physical examination is imperative to guide diagnostic investigations.
-
Hypoactive delirium is probably more common than the hyperactive type but is frequently missed. Overall, 30% to 60% of all cases of delirium are thought to remain undiagnosed.
-
Hypoadrenalism and hypothyroidism directly and indirectly through hyponatraemia could contribute towards the development of delirium.
-
The presence of more than one anterior pituitary hormone—target hormone axis deficiency—should raise the possibility of pituitary insufficiency.
-
Hypopituitarism is an uncommon and under investigated disease among the elderly, since its symptoms are often non-specific and can be ascribed to ageing and comorbidities.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.