Article Text

Abstract
Objectives Catastrophic haemorrhage is a leading cause of morbidity and mortality in trauma, in both military and civilian settings. There are numerous studies looking at the effectiveness of different haemostatic agents in the laboratory but few in a clinical setting. This study analyses the use of haemostatic dressings used in patients injured on the battlefield and their association with survival.
Method A retrospective database review was undertaken using the UK Joint Theatre Trauma Registry from 2003 to 2014, during combat operations in Iraq and Afghanistan. Data included patient demographics, the use of haemostatic dressings, New Injury Severity Score (NISS) and patient outcome.
Results Of 3792 cases, a haemostatic dressing was applied in 317 (either Celox, Hemcon or Quickclot). When comparing patients who had a haemostatic dressing applied versus no haemostatic agent, there was a 7% improvement in survival. Celox was the only individual haemostatic dressing that was associated with a statistically significant improvement in survival, which was most apparent in the more severely injured (NISS 36–75).
Conclusion We have shown an association between use of haemostatic agents and improved survival, mostly in those with more severe injuries, which is particularly evident in those administered Celox. This supports the continued use of haemostatic agents as part of initial haemorrhage control for patients injured in conflict and suggests that civilian organisations that may need to deal with patients with similar injury patterns should consider their use and implementation.
- trauma management
- accident & emergency medicine
- wound management
Statistics from Altmetric.com
Haemorrhage is one of the leading causes of morbidity and mortality in trauma patients.
Studies have tested haemostatic agents in the laboratory environment but there are very few looking at its use in the clinical setting.
We reviewed the use of haemostatic agents in injured patients during the conflicts in Iraq and Afghanistan who presented to deployed UK medical treatment facilities.
We showed an association between the use of haemostatic agents and improved survival, mostly in those with more severe injuries, which is particularly evident in those administered Celox.
Haemorrhage is a leading cause of mortality in major trauma patients on the battlefield, second only to traumatic brain injury (TBI).1 Several studies have found it to be the most common cause of potentially preventable death.2–4 In one analysis of US military casualties, over 90% of the potentially survivable injuries were associated with haemorrhage,2 and of these patients the most common regions affected were truncal (67.3%), junctional (19.2%) and extremity (13.5%).2
Recent terrorist attacks have highlighted that the battlefield is no longer confined to traditional boundaries of conflict zones, and the injury patterns they produce are similar to military patients injured in war. During the recent terrorist attacks in London and Manchester, large numbers of casualties sustained injuries where haemorrhage was a major component, highlighting the need for methods of haemorrhage control to be made available to civilian pre-hospital clinicians.5 6
The introduction of combat tourniquets has improved survival from extremity haemorrhage.7 The first step in the treatment of external haemorrhage is to apply direct pressure to the wound, followed by the application of a tourniquet if the anatomical site of the injury allows it.8 Junctional haemorrhage affects areas where the trunk of the body meets the limbs. It is difficult to control haemorrhage at these points as, by definition, tourniquets cannot be used to provide circumferential pressure above the wound, and so we rely solely on directly applied pressure. Another study from the United States of America analysing patients injured in Iraq and Afghanistan between 2001 and 2010 identified haemorrhage control of this type as the most frequent intervention.9
Haemostatic agents can be used as an adjunct to a tourniquet or direct pressure. The UK Armed Forces introduced haemostatic agents into use in 20043 and since then, three haemostatic agents have been used, in various forms: Quickclot, Hemcon and Celox. Quickclot is a factor concentrator that contains an inert material called kaolin.10 Celox and Hemcon are both mucoadhesive agents that contain the active adhesive component chitin, found in shellfish.10 Celox has become the sole product currently used by the UK Armed Forces. Several studies have demonstrated the effectiveness of haemostatic agents in haemorrhage control,3 11–13 but there are very few describing the use of haemostatic agents in the clinical military setting.
The aim of this study was to provide a descriptive analysis of the use of haemostatics in major trauma patients on the battlefield. We examined patient demographics, levels of injury severity and associated rates of survival.
Methods
We undertook a retrospective database analysis using the UK Joint Theatre Trauma Registry (JTTR). The JTTR is a database containing information on all patients who activated a trauma call and were treated by the UK Defence Medical Services in Iraq and Afghanistan, including UK and Coalition military and local nationals. Data are collected from a combination of clinical notes, trauma charts and post mortems where applicable. Entries are submitted electronically, where possible, with hard notes accompanying patients on repatriation to the UK for entry onto the registry. The JTTR was formerly maintained by the Academic Department of Military Emergency Medicine at the Royal Centre for Defence Medicine, Birmingham and latterly by the Defence Analytical Services Agency.
We used the New Injury Severity Score (NISS) to allow analysis of levels of injury severity. This system assigns each injury a score using the military adjusted Abbreviated Injury Scale. Each injury is categorised by anatomical region and given a score from 1 (minor injury) to 6 (maximum lethal injury). It then adds the sum of the squares of the three most severe injuries to form the NISS. The NISS ranges from one up to most severe 75; if any regional score is 6 then the NISS is automatically calculated as 75 for that patient.14 We used a score of over 15 to identify major trauma patients.15
A search of the JTTR was undertaken to identify patients with an NISS of 15 or more between 2003 and 2014, through the conflicts in Iraq and Afghanistan. Patient demographics, survival, injuries and treatment with Quickclot, Hemcon and Celox were recorded. Excel (Microsoft) was used to manage the data and SPSS version 23 (IBM) was used to perform statistical analysis on the results obtained. Direct comparison was undertaken using independent t-test and comparison of categorical data was done using Pearson’s χ2 test. Where the number of cases did not meet the minimum criteria for χ2 test, Fisher’s exact two-sided test was used. Three subgroups were analysed, defined by NISSs of 16–35, 36–55 and 56–75, to enable comparison of haemostatic use in increasing severity of injury. Patients were eligible for inclusion if they were injured in the Iraq or Afghanistan conflicts and had a NISS of greater than or equal to 15. They were excluded if they had no NISS recorded or if they had a NISS of less than 15. Those who had multiple haemostatic agents used on them were also excluded to allow comparison between individual agents.
Results
A total of 3792 patients were eligible for analysis of which 3475 had no haemostatic agent used and 317 had a single haemostatic agent used (Figure 1). There was a mean age of 24.8 years; most patients were men, and there was an median NISS of 36.0. Also, 64.6% of patients survived. Table 1 shows the population characteristics.
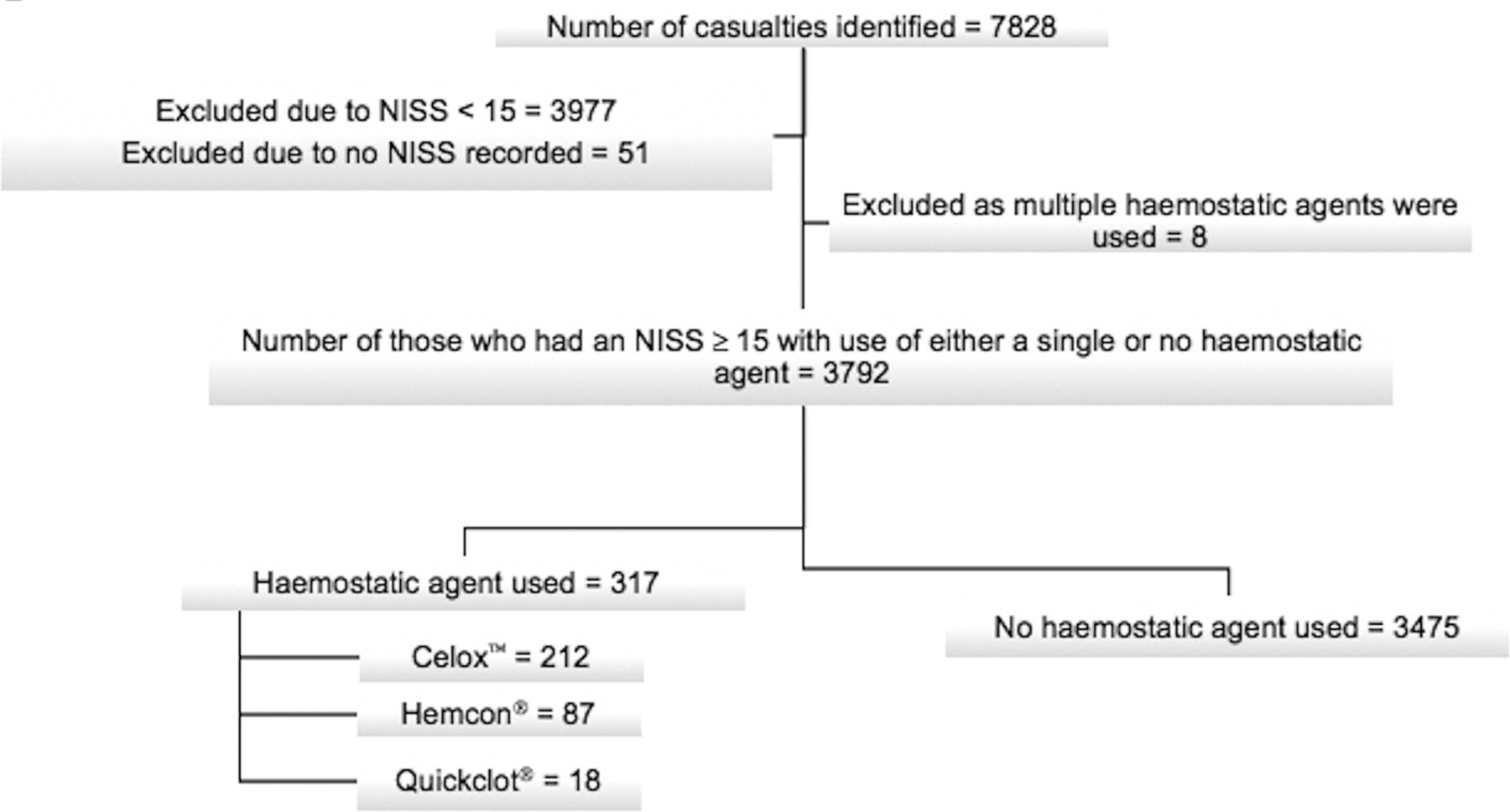
Patient selection criteria. NISS, New Injury Severity Score.
Population characteristics
Blast and gunshot wounds accounted for over 98% of injuries (65.7% and 32.6%, respectively). Table 2 shows the comparison of variables across the two groups. There was no difference in mean age or NISS between the haemostatic agent and no haemostatic agent groups. There is an associated statistically significant increase in survival between groups.
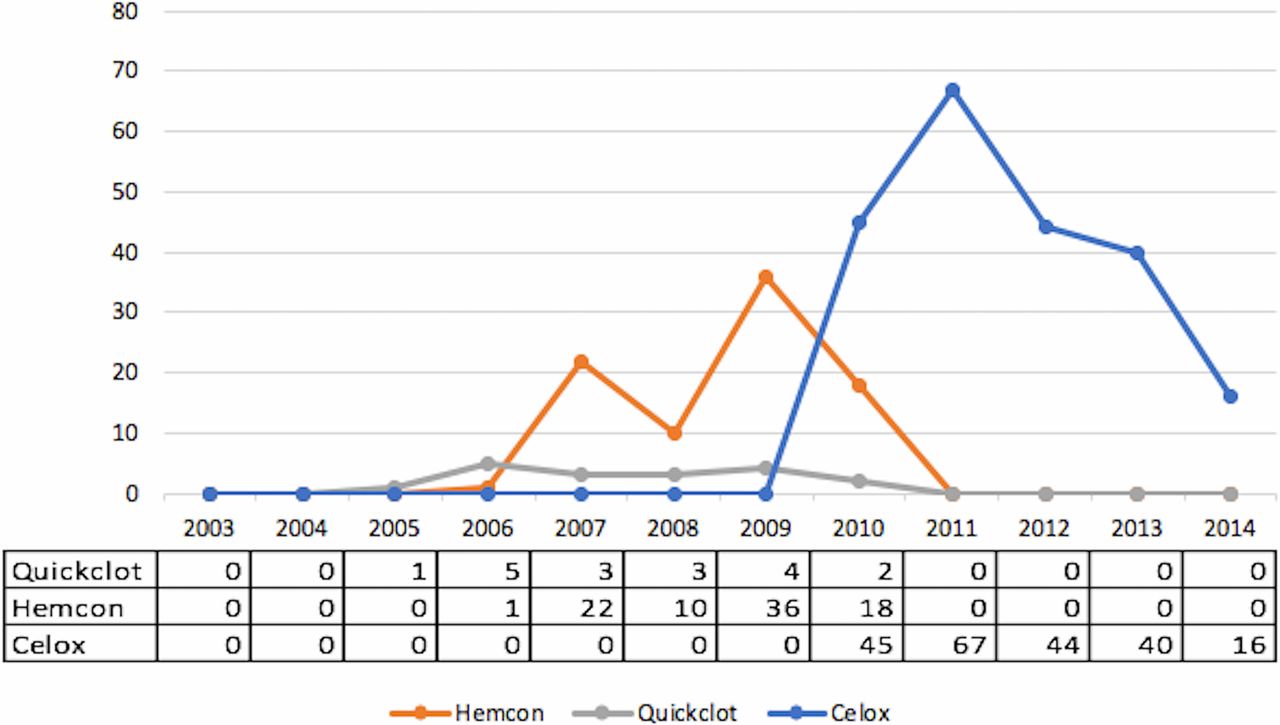
Figure 2 shows the temporal use of each haemostatic agent per year. Initially, Hemcon and Quickclot were most commonly used, but since 2010, the most common agent used has been Celox.
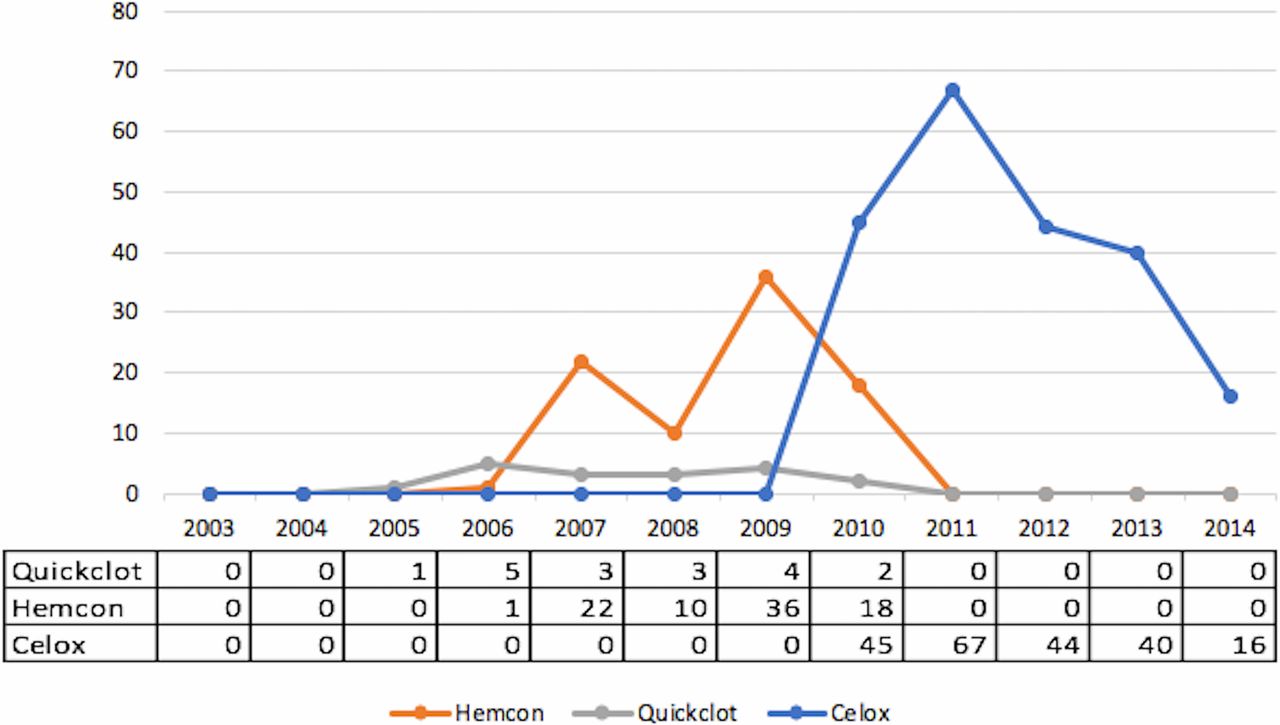
Quantity of each haemostatic agent used each year.
Comparison of variables across the two study groups
Table 3 shows a comparison of no haemostatic agent to any haemostatic agent and then each individual haemostatic agent compared with no haemostatic agent. There is a difference in survival between the two comparison groups, with an associated increase in survival when comparing any haemostatic agent used with none, and in the most severely injured, NISS range 56–75. Individual analysis of each haemostatic agent showed no associated increase in survival for Hemcon or Quickclot; Celox demonstrated an increase in survival overall, most evident in those with a NISS over 35.
Figure 3 shows the percentage difference in survival between all compared groups,with the associated statistically significant increases in survival underlined.

{kind=link}
{kind=link}
{kind=link}
Percentage increase in survival (underlined: p<0.05). NISS, New Injury Severity Score.
Comparison of survival between those receiving haemostatic agents and those who did not, with different injury severity
Discussion
This study has defined for the first time the use of haemostatic agents on patients injured in Iraq and Afghanistan, and shows an association between the use of haemostatic agents and survival. This supports the continued use of haemostatic agents as part of initial haemorrhage control for patients injured in conflict and suggests that civilian organisations that may need to deal with patients with similar injury patterns should consider their use and implementation.
This study confirms that the predominant mechanisms of injury in patients injured in the conflicts in Iraq and Afghanistan were explosion and gunshot wounds.1 16 It has been suggested that the mechanism of injury affects acute coagulopathy of trauma in combat casualties, with one study reporting that patients injured by explosive devices have more coagulopathy when compared with gunshot wounds, even in those with similar injury severity scores.17 Recent terror attacks around the world have made these injury mechanisms and injury patterns more common within the civilian population.5 6
The use of haemostatic dressings is a key step in the management of catastrophic haemorrhage. Direct pressure should be applied to a haemorrhaging wound, followed by a tourniquet if the wound is suitable. Tourniquets were introduced as personal first aid in April 2006.18 Their increase in availability and training, and therefore increased effective frontline use, has had an impact on pre-hospital care and in turn on patient outcome. Kelly et al highlighted that tourniquets were a major factor in the reduction of mortality in their review of injuries and causes of death in Iraq and Afghanistan.7
The next step in the management of haemorrhaging wounds is the application of a haemostatic dressing. Kozen et al compared Quickcot, Celox and Hemcon in an animal model of haemorrhage and found that Celox reduced bleeding to 0%, Hemcon to 33% and Quickclot 8% compared with 83% in normal gauze.19 A case series from Afghanistan in 2011 looked at the use of Celox in massive traumatic bleeding in gunshot wound patients. It found that 18 out of 21 gunshot patients had clot formation within a minute on first application with the other three requiring a second application to stop arterial bleeding.20 In our cohort, we found a statistically significant associated increase in survival with the use of Celox vs no haemostatic agent.
In this study population, Quickclot and Hemcon were used more commonly initially with Celox being used more frequently over the latter years. Celox was introduced as the sole UK haemostatic agent of choice during the Afghanistan conflict. Quickclot and Hemcon products have been shown to be effective in trauma settings in both civilian and military environments and have previously been part of the Tactical Combat Care guidelines.21 The UK military used differing versions of Hemcon and Quickclot during the study period, and we are unable to state which exact product version was used in each patient from the data available, limiting that aspect of analysis of these specific agents. Due to these limitations, this study is unable to make a comparison between the three haemostatic agents used.
When comparing outcomes in those who had haemostatic dressings applied, Celox was associated with a statically significant increase in survival when compared with those who did not receive any haemostatic agent. There was an increase in survival in the higher severity injuries with a NISS of 36–75, possibly due to the nature of the wounds sustained being amenable to haemorrhage control rather than simple interventions.
Limitations
This study is limited by the nature of the database from which the data were extracted. It was not possible to identify the anatomical area of application of the haemostatic agent from the data available.
Although an association may be apparent, no causation can be attributed due to the nature of the study. An additional confounder was that in patients who were not administered haemostatic agents, different injury patterns and body regions may be more likely to cause death, even when matched for NISS, for example those with severe head injuries.
Conclusion
This study has defined the use of haemostatic agents in the conflicts in Iraq and Afghanistan, among the population of patients presenting to deployed UK medical treatment facilities. There is an association between the use of haemostatic agents and improved survival, mostly in those with more severe injuries, which is particularly evident in those administered Celox.
Acknowledgments
The Clinical Information Exploitation Team and Defence Statistics Health are thanked for collecting, collating and identifying the appropriate data for this paper.
References
Footnotes
Contributors All authors have made the appropriate level of contribution to be listed as authors in the order stated.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; internally peer reviewed.