Article Text

Abstract
Objective: To describe the safety profile of emergency airway management when performed by a prehospital team consisting of a doctor and a paramedic. Success rates, the incidence of difficult airways and the ability of prehospital doctors to determine a difficult airway are reported.
Methods: A prospective audit and descriptive study of three Australian helicopter emergency medical service (HEMS) bases, over a 9-month period. Doctors completed questionnaires regarding the number of endotracheal intubation (ETI) attempts on patients transported intubated and ventilated, Cormack and Lehane view of the cords during laryngoscopy and the anticipated and actual ease of ETI.
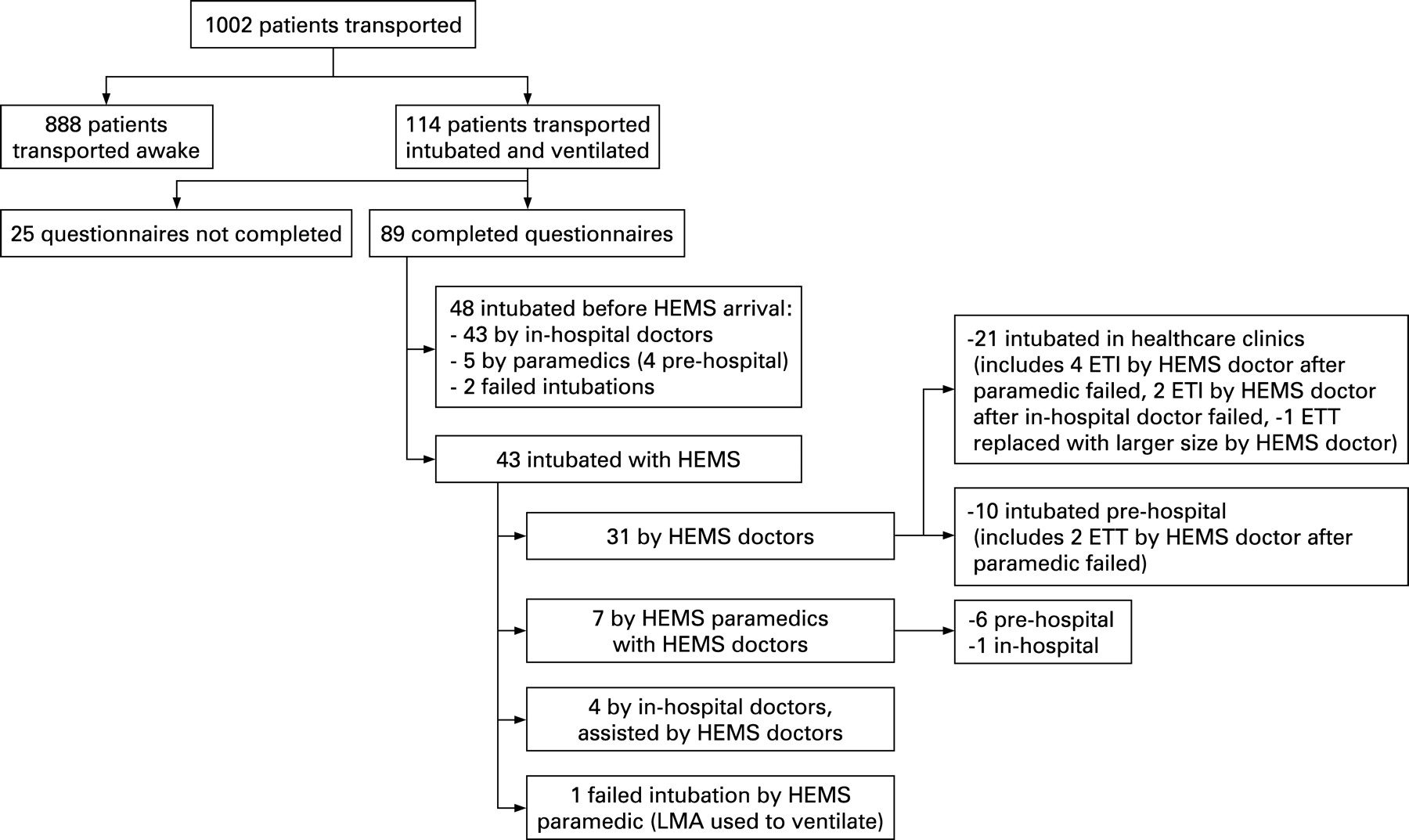
Results: A total of 114 (11.4%) patients transported by the HEMS was intubated and ventilated. Study questionnaires were completed on 89 of the 114 cases (78.1%), of which 32 (36%) were trauma related. HEMS were involved with 43 (48.3%) of the 89 intubations and performed 12.4% (n = 11) out of hospital. The HEMS ETI success rate was 97.6%. No surgical airways were performed. The actual incidence of difficult airways was higher (n = 4, 9.3%) than the anticipated incidence (n = 1, 2.3%). Six patients (14.0%) were successfully intubated by the doctor after the paramedic failed.
Conclusions: Well-trained doctor paramedic teams, utilising standardised operating procedures, can safely perform rapid sequence induction and ETI in the prehospital and emergency environment. However, prehospital doctors are not always able to anticipate a difficult airway. The complication rate was similar to that in hospital emergency departments and to that of other physician-led HEMS.
Statistics from Altmetric.com
Airway management is a priority during the resuscitation of severely sick or injured patients. For certain patients, endotracheal intubation (ETI) requires the administration of anaesthetic drugs and muscle relaxants as part of rapid sequence induction (RSI). Prehospital RSI offers early airway protection and controlled ventilation, which are essential in the management of certain patients, in particular the patient with serious head injuries.1–3 Prehospital anaesthesia also allows the prehospital team to manage agitated patients better, such as those with head injuries and a relatively high Glasgow coma scale score.4 Although there is evidence that RSI in the prehospital setting can be performed safely when carried out by properly trained practitioners5–9 the risks are well recognised.10–14
Prehospital anaesthesia and airway management confronts emergency teams with complex challenges and is a skilled technique that requires considerable training and experience. In comparison with inhospital, prehospital airway management has been reported as more difficult.15 Challenges to intubation in a prehospital setting include non-fasted, awake or combative patients. Other physical factors thought to create a difficult intubation include blood, vomit and debris in the upper airway, difficult access to the patient and surrounding conditions such as inadequate lighting, excessive noise, limited equipment and monitoring and lack of skilled help. Despite these factors, the same high standards for successful intubation demanded in the hospital environment must be applied to the prehospital setting to ensure positive outcomes.
The purpose of this study was to describe the safety profile of emergency airway management when performed by a prehospital team consisting of a doctor and a paramedic. We report ETI success rates, the incidence of difficult airways and the difference between anticipated and actual difficult airways as perceived by prehospital doctors.
METHODS
This was a prospective, descriptive audit of three CareFlight Queensland helicopter emergency medical services (HEMS) over a 9-month period (21 October 2006 to 15 July 2007). The participating HEMS included Emergency Management Queensland (EMQ) Townsville and Cairns, and CQ Rescue Mackay. The participating HEMS are medically staffed by CareFlight Medical Services (CMS), part of the CareFlight Group, a medical rescue and retrieval service operating in Queensland, Australia. The CareFlight HEMS missions include primary responses, search and rescue and interhospital transfers. The majority of interhospital transfers are from small healthcare clinics, akin to the resource-poor prehospital environment.
The flight crew usually consists of a pilot, one or two crew members, a doctor and a paramedic. The medical team consists of a consultant or retrieval registrar (senior emergency, anaesthetics or intensive care registrars) and a senior or intensive care paramedic from Queensland ambulance service. Neonatal interhospital transfers (approximately <5 kg) are performed by specialised retrieval teams from the receiving hospitals and CMS doctors are generally not involved. It is the doctors’ responsibility to carry out an initial assessment and resuscitation of the patient on-scene before transporting them to the nearest or most appropriate hospital. Following risk benefit analysis, RSI is carried out using a statewide standard operating procedure (see appendix available online only).
The ETI study questionnaire was developed by one of the authors (EO’L) and was completed by the HEMS doctor immediately after each mission. The forms were anonymised and the data collected on the ETI questionnaire included patient demographic information, operator level, location and reason for ETI, anticipated and actual ease of ETI, laryngoscopic view as determined by Cormack and Lehane (C&L) grades I to IV, number of ETI attempts and if any complications were experienced.
The analysis of the results was subsequently carried out by doctors from a different base (CMS Gold Coast). Analysis between all HEMS was performed using one-way analysis of variance for continuous data (age) and Kruskal–Wallis χ2 tests for grouped data (gender, diagnosis, number of attempts). Analysis between one HEMS and another was performed using the Mann–Whitney U test. Unless otherwise indicated, analysis for number of ETI attempts, laryngoscopic view and ease of ETI are based on 43 transfers in which CMS performed ETI. Two-sided p values are reported with a probability value of less than 0.05 considered statistically significant.
RESULTS
A diagram of the sampling process is displayed in fig 1. During the 9-month study period, the three participating HEMS bases transported a total of 1002 patients. Of the 1002 patients, 114 were intubated (11.4%). Most (89, 78%) had completed questionnaires that were utilised for data analysis purposes. (The diagnosis was not recorded on three of the 89 questionnaires; the age was omitted from three and the gender from another one questionnaire.)

{kind=link}
Table 1 displays the characteristics of HEMS transports of intubated patients for each base. Townsville recorded most transports, followed by Cairns and then Mackay. The majority of transports were men in their mid-forties. There were no significant differences for transported patients between bases, in terms of their age (p = 0.61), gender (p = 0.79), or diagnosis (p = 0.96). The number of intubated and ventilated transports differed significantly between bases. At HEMS Mackay (3.1%) intubated and ventilated transfers were significantly lower than at the two other HEMS (7.6% at HEMS Townsville, p = 0.04, and 15.7% at HEMS Cairns, p<0.001).
The overall success of the HEMS ETI attempts was 97.6%, but all of the patients were successfully ventilated. Most patients (30, 69.8%) were intubated successfully on the first attempt, 23.3% the second and 2.3% on the third attempt (table 2). One case required more than three attempts at ETI: this patient, assessed as having a moderately difficult airway, was found to have a grade III view during laryngoscopy. There was one failed intubation with possible aspiration by a HEMS paramedic. This followed three attempts at intubation with a bougie in a patient who had sustained a head injury. An alternative airway device (size 5 laryngeal mask airway) was inserted to facilitate ventilation for the transfer. No patient within the study group required a surgical airway. The indications for ETI are also shown in table 2, the majority being airway protection.
The number of ETI attempts and C&L16 view of the cords are displayed in table 3. Whereas most cases (36, 85.7%) were reported to have a good view (C&L I /II) of the cords, 33.3% (n = 12) of these cases required more than one attempt at ETI. One case of unsuccessful ETI was reported for a patient who had a C&L laryngoscopic view of IV.
Anticipated and actual ease of ETI was reported (table 4). The majority of those cases thought to be easy had grade I and II C&L views and required fewer attempts than those thought to be moderate or hard; 9.3% (n = 4) of ETI were more difficult (reported as hard) than anticipated (2.3%, n = 1).
DISCUSSION
The benefit of prehospital RSI and ETI are the subject of much debate. ETI secures the airway and is a priority in the resuscitation of the trauma patient. Poorly performed prehospital RSI can be dangerous, and therefore RSI should only be performed by appropriately trained, competent practitioners.17 This study identified differing numbers of transports between HEMS bases. This probably represents the unique nature of the HEMS work for each region, the transport times to, and the level of, receiving hospitals as well as the skills of the HEMS crew members.
Anticipating a difficult airway
Results from this study indicate that HEMS doctors were not always able to anticipate a difficult airway. Compared with inhospital, prehospital airway management can be made more difficult due to a number of factors, including blood, vomit and debris in the upper airway, hypersalivation, anatomical reasons, difficult access to patient, limited equipment and monitoring, lack of skilled help and the surrounding conditions such as inadequate lighting and excessive noise.18 Combes et al15 highlighted several factors that were independently associated with difficult intubation. These included a history of ear, nose and throat neoplasm or surgery, obesity, facial trauma, operator’s status and operators’ position during intubation.15
Incidence of difficult airways
The actual incidence of subjectively assessed difficult airways in this study was 9.3% (n = 4). Prehospital difficult intubation is poorly defined in the prehospital environment and the incidence has been reported to be between 5% and 50%.15 A previous study by emergency physicians5 reported difficulty with 65% of trauma patients in the prehospital setting; however, all these patients had a hard collar in situ. When difficult tracheal intubation is more precisely defined using the intubating difficulty score, the reported incidence is lower (16%) in prehospital emergency medicine.19 Successful ETI at first attempt has been reported to be between 57.9% and 98.9%.18 Wang and Yealy20 found, as in this study, that more than 30% of their patients received more than one attempt and they suggest that a limit of three attempts offers “reasonable opportunity for accomplishing ETI within the constraints of the out of hospital environment”. Combes et al15 found that if prehospital airway management is standardised and performed by well-trained practitioners, the incidence of difficult ETI is 7.4% and the failure rate is low (0.1%). The systematic application of a predefined algorithm designed to manage the unanticipated difficult airway was reported to have possibly contributed to the low incidence of difficult airways observed.15
Success rates
Inhospital failed intubation rates quoted within the anaesthesia literature range from 0.1% to 0.4%, with the emergency department rate being slightly higher at approximately 1%.21 22 Therefore, the prehospital success rate needs to be 99% in order for the practice to be accepted and result in positive patient outcomes. Our overall (97.6%) and prehospital (100%) successful intubation rate is comparable with other studies conducted overseas evaluating physician prehospital ETI;15 18 23 24 however, our numbers were smaller in comparison.
A study from Germany18 suggested that their 100% success rate of prehospital intubations was due to a small number of participating anaesthetists and paramedics who worked together regularly as a team, who were all trained in trauma. The rate of failed intubations and complications in our study group would have been much higher without the presence of an appropriately trained and skilled critical care doctor in the HEMS team. In eight of the 89 cases (9%), the HEMS doctor was able to intubate the patient successfully after either the paramedic or inhospital doctor failed. Paramedic-led RSI is controversial and has been associated with increased mortality,9 11 12 which again illustrates the importance of training and working as a team.
Improving success
Combes et al,15 like others, observed that intubation conditions were not influenced by the speciality of the prehospital care provider, ie, emergency medicine versus anaesthetist. However, they did find that more frequent difficult intubations arose when more junior physicians were intubating.15 This reinforces the fact that education is a major determinant of practical performance when it comes to intubation. Patient selection is important and the presence of an appropriately trained and skilled doctor helps by targeting those patients that would benefit from early intubation and targeted ventilation.
The skill of airway management has been shown to decline after initial training.21 However, independent practice with feedback has been shown to be effective in maintaining performance. Some authors suggest an ongoing requirement to perform a certain number of intubations over a certain period in order to maintain competency.17 21 Improving prehospital RSI success requires continual combined doctor and paramedic training to improve techniques and develop a planned sequential approach to overcome difficult airway scenarios. Standardised protocols or standard operating procedures have been found to improve intubation success.23 Training in the use of end tidal carbon dioxide detection and adjuncts such as the bougie and the use of external laryngeal manipulation or backwards upwards rightwards pressure to improve laryngoscopic view is recommended. Commitment to quality assurance and performance review is important21 and our HEMS doctors and paramedics attend weekly training and audit sessions. CMS were informed of the results of the audit and the data have been utilised for service improvement.
Study limitations
Given that the final dataset was relatively small (43 HEMS ETI), even one or two failed intubations without a completed questionnaire could skew the study results. The 78.1% response rate was, however, more than the 65% that is considered sufficient when collecting questionnaire data25 and almost all returned questionnaires were complete. Possible reasons for the unreturned questionnaires may be due to time pressures or the use of locum doctors who may not have been aware of the study. The majority of unreturned questionnaires was from the busiest HEMS base in the study (Townsville). The relatively small dataset also limited the level of data analysis that could be performed; however, the study was designed as a pilot to be conducted over a set number of months.
The number of ETI attempts reported may be influenced by an underreporting bias. Retrospective completion of the forms may also have influenced the reported grade of the laryngoscopic view following a difficult intubation. The study questionnaire did not examine conditions, the use of intubation aides, examination and vital signs or patient follow-up.
CONCLUSION
Well-trained doctor paramedic teams, utilising standardised operating procedures, can safely perform RSI and ETI in the prehospital and emergency environment. The overall 97.6% successful intubation rate in this study may be attributed to the HEMS medical team model. However, prehospital doctors are not always able to anticipate a difficult airway. The complication rate was similar to that in hospital emergency departments and to that of other physician-led HEMS. A larger study containing comprehensive safety and outcome elements regarding HEMS transports of ETI patients is recommended in order to guide clinical practice and enhance patient safety in the HEMS environment.
Acknowledgments
The authors would like to thank Dr Gerben Keijzers from the Gold Coast Hospital for his assistance with data analysis and manuscript review.
REFERENCES
Supplementary materials
web only appendix 26/1/65
Files in this Data Supplement:
Footnotes
Additional appendix is published online only at http://emj.bmj.com/content/vol26/issue1
Competing interests: None.
Contributors: MG contributed to the acquisition of data, data analysis, drafting and submission of the manuscript; EO’L contributed to study concept and design, acquisition of data and critical revision of the manuscript; MF contributed to critical revision of the manuscript; JC contributed to data analysis and manuscript review; MH contributed to study concept and design, critical revision of the manuscript and study supervision; DYE contributed to study concept and critical revision of the manuscript.
Study locations: Cairns base: EMQ, Hanger 12, Bushpilot Avenue, Aeroglen, Queensland 4870, Australia; Townsville base: Queensland Rescue, 114 Gypsie Moth Court, Townsville Airport, Townsville, Queensland 4350, Australia; Mackay base: CQ Rescue, East Boundary Road, Mackay Airport, Mackay, Queensland 4740, Australia; Gold Coast base: CareFlight, 44 Eastern Avenue, Bilinga, Queensland 4225, Australia.