Article Text

Abstract
Objectives: To review the injuries resulting from the attenuated energy projectile (AEP) in patients who present to emergency departments.
Method: Review of case notes of patients presenting with injuries caused by the AEP after three episodes of serious civil disturbance in Northern Ireland from July to September 2005.
Results: 14 patients with 18 injuries were identified and included in the study. All patients were male, with an average age of 26.3 years. There were six injuries above the level of the clavicle, to the head, face or neck. There were three chest injuries, seven lower limb injuries and two upper limb injuries. There were no abdominal injuries. Seven patients required hospital admission. Five patients required surgical intervention. One patient required protective, elective intubation and one patient required the insertion of a chest drain.
Discussion: Although the study numbers were small, 33.33% of injuries were to the head and neck and 16.67% of the injuries were to the chest. The AEP was introduced as a replacement for its predecessor, the L21A1 plastic baton round, because of a theoretical risk of serious or even life threatening head injury from this projectile in certain circumstances. However, in this first survey of its usage, 50% of the injuries presenting to hospital were to the face, neck, head or chest. This injury pattern was more in keeping with older plastic baton rounds than with the L21A1.
- AEP, attenuated energy projectile
Statistics from Altmetric.com
The attenuated energy projectile (AEP) is the most recent projectile to be developed as a less lethal system for use against violent individuals in the management of civil unrest or conflict. It has been issued to police forces in the UK and to the police force and British Army in Northern Ireland, and has been available since 21 June 2005. It replaced the L21A1 plastic baton round, which itself had been in use since May 2001.1
The L21A1 round was introduced because of a belief that it would be less likely to cause life-threatening injury than its predecessor, the plastic baton round, when used by appropriately trained police officers. However, in certain circumstances—for example, high-energy ricochets—the potential for more serious and life-threatening head injury seemed to increase. Once this conclusion was reached by the Defence Scientific Advisory Council, work was undertaken under the direction of the Northern Ireland Office to develop a weapons system that would offer energy-attenuating features and ricochet characteristics different from the L21A1. This led to the development of the AEP. The AEP is a projectile designed to deliver an impact to an individual, to dissuade or prevent an intended course of violent action, and, thereby mitigate the threat to law-enforcement personnel and members of the public. It is not intended to cause serious or life-threatening injury.2
The AEP was designed to be more accurate, safer and reduce the injury potential compared with the L21A1, and especially to reduce the clinical consequences of an injury to the head. It does not fragment, which in itself reduces the risk of accidental injury and the potential for ricochet injury.
The AEP was designed to be fired from the L104A1 gun using the same XL1 18E3 optical sight as the old L21A1 round. There were no changes in the guidelines regarding its use.2
The AEP is made of polyurethane (owing to its temperature stability and the possibility of tightly controlling the material properties). The crumple zone is polyurethane, with an air gap in the nose. Its dimensions are similar (10×3.7 cm) to its predecessor, as is its weight (98 g). The mean velocity is 72 m/s. It delivers a slightly higher kinetic energy on initial impact than its predecessor, the L21A1 (254 J upon striking its target compared with 244 J), although its design means that there is less kinetic energy transfer once the target has been struck.
The L21A1 was last used in Northern Ireland in September 2002, and the AEP was first used in July 2005. It is important to point out that although the AEP had already been fired on a number of occasions by police forces in Great Britain, it may be used there against specific individuals who pose a major threat whereas in Northern Ireland, it is used against individuals in circumstances of serious public disorder and riot.
METHODS
Patient records were collected retrospectively from emergency departments covering the areas in which there had been rioting and where AEPs had been fired by the security forces. Four departments reported seeing patients with injuries said to be caused by AEPs.
All sets of notes were reviewed, and the following data were collected: age, sex, site of injury and whether or not the patient required hospital admission. For all patients, an injury score was then calculated using the Abbreviated Injury Scale.3 Injuries are ranked on a scale of 1–6, with 1 being minor, 3 serious and 6 an unsurvivable injury. This represents the “threat to life” associated with an injury and is not meant to represent a comprehensive measure of severity.
RESULTS
The notes of 14 patients were collected from the four departments that reported seeing patients with injuries said to be caused by AEPs. These 14 patients had sustained 18 injuries attributable to AEPs (2 patients were struck on 2 contiguous regions of the body by 1 AEP or by >1 AEP, and another patient was struck on the same region by 3 AEPs). All the patients were male. Seven of the patients required hospital admission related to the injury inflicted by the AEP. An eighth patient was admitted because of concomitant injuries not attributable to an AEP. One patient was admitted to an intensive care unit after protective endotracheal intubation. The patients were aged 14–45 years, with a mean age of 26.3 years.
Listed below are the injuries of patients admitted to hospital:
-
Patient 1: closed mandibular fracture/neck haematoma
-
Patient 2: compound Le Fort fracture
-
Patient 3: neck haematoma
-
Patient 4: compound fractures—frontal bone, infraorbital bone, globe rupture
-
Patient 5: bilateral frontal sinus fractures, bilateral frontal lobe contusions
-
Patient 6: compound nasoethmoidal fracture, medial orbit fracture, traumatic mydriasis
-
Patient 7: traumatic pneumothorax
Listed below are the injuries of patient discharged from hospital:
-
Patient 8: chest wall contusion, thigh contusion
-
Patient 9: groin contusion
-
Patient 10: thigh contusion
-
Patient 11: head/foot contusion
-
Patient 12: elbow contusion
-
Patient 13: wrist fracture/chest wall contusion
Patient 14 was admitted because of serious injuries not attributable to an AEP, but had three lower limb contusions caused by an AEP.
None of these patients were readmitted after discharge.
Table 1 shows the Abbreviated Injury Scale scores of the injuries sustained. As previously stated, one patient required elective intubation, one required surgical enucleation, five required maxillofacial intervention, one required insertion of a chest drain and one required overnight observation only. None of the lower limb patients with injuries required active intervention. The patient with a chest wall injury and wrist fracture was to be admitted for observation, but discharged himself against advice. Neither of the two patients with chest wall contusions had an underlying pulmonary contusion.
Abbreviated Injury Scale scores of the injuries sustained by patients
One patient was excluded from the study as he gave two different accounts of how his injury had occurred: that he had been hit by an AEP and also that he had sustained the injury while playing football.
DISCUSSION
Clinically, the nature of injury caused by the AEP is blunt trauma. Although the kinetic energy of the AEP on initially striking its intended target is slightly greater than that of the L21A1, its design means that after impact, there is less transfer of kinetic energy. The clinical description of the visible injury caused remains unchanged—that is, about a 4-cm diameter circular abrasion with surrounding contusion.
The numbers in this study are small, but we believe important in view of the fact that the AEP was developed and introduced because of the theoretical risk that its predecessor, the L21A1, might cause serious or fatal head injury. Therefore, it is important to note that 6 out of the 14 patients presented with injuries to the face, neck or head. A previous publication4 reviewing injuries after impact from the L21A1 noted that none of the patients presenting had sustained injuries in these body regions. To our knowledge, in about 20 incidents in Great Britain in which the L21A1 was fired, there were no reports of head injuries and deaths. The small number of patients included in this study does not allow for statistical comparison with previous studies. However, with 36.67% of patients with injuries above the clavicle, the injury pattern is more in keeping with those described in previous studies by Sheridan and Whitlock,5 Rocke,6 Ritchie7 and Steele et al,8 which showed 40.5%, 41.4%, 23% and 19.2%, respectively, of patients presenting with injuries above the clavicle. It is important to note that 16.67% of injuries sustained were to the thoracic region and that there were no abdominal injuries. There was only one bone fracture, and in none of the injuries to the extremities was there serious soft tissue damage.
The 14 deaths attributable to rubber or plastic bullets in Northern Ireland have all been due to head or chest trauma.
The stated objective for the AEP development and introduction was to decrease the possible risk of serious or fatal head injury. Although no deaths were attributable to the use of the AEP, a combined total of 50% of the injuries sustained were to the thorax or above the clavicle. In this context, is it fair to ask if there is such a thing as a “safer” head injury? It is clear that the AEP requires ongoing evaluation, and it is too early to conclude that it provides a safer alternative to the L21A1 (fig 1).
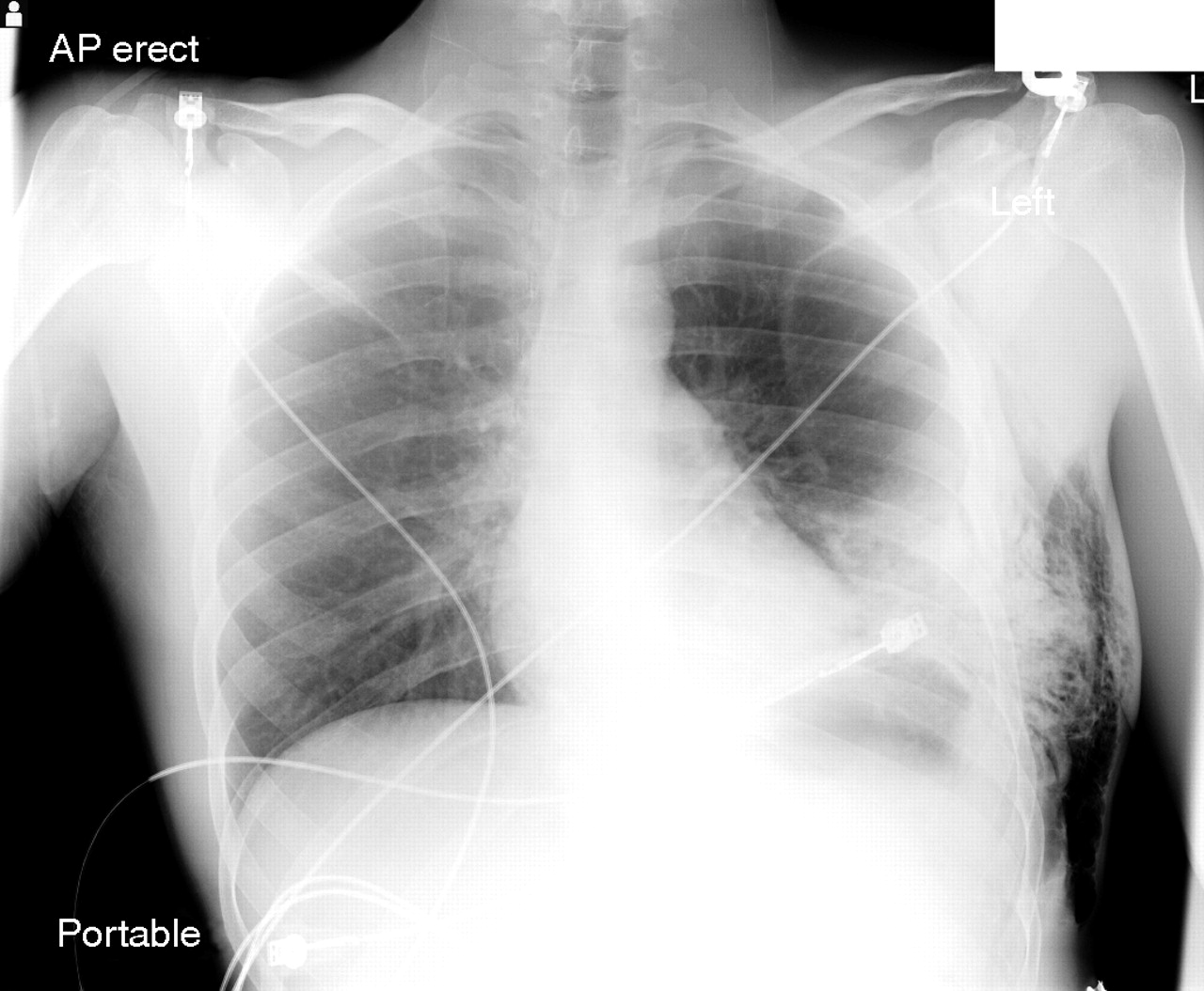
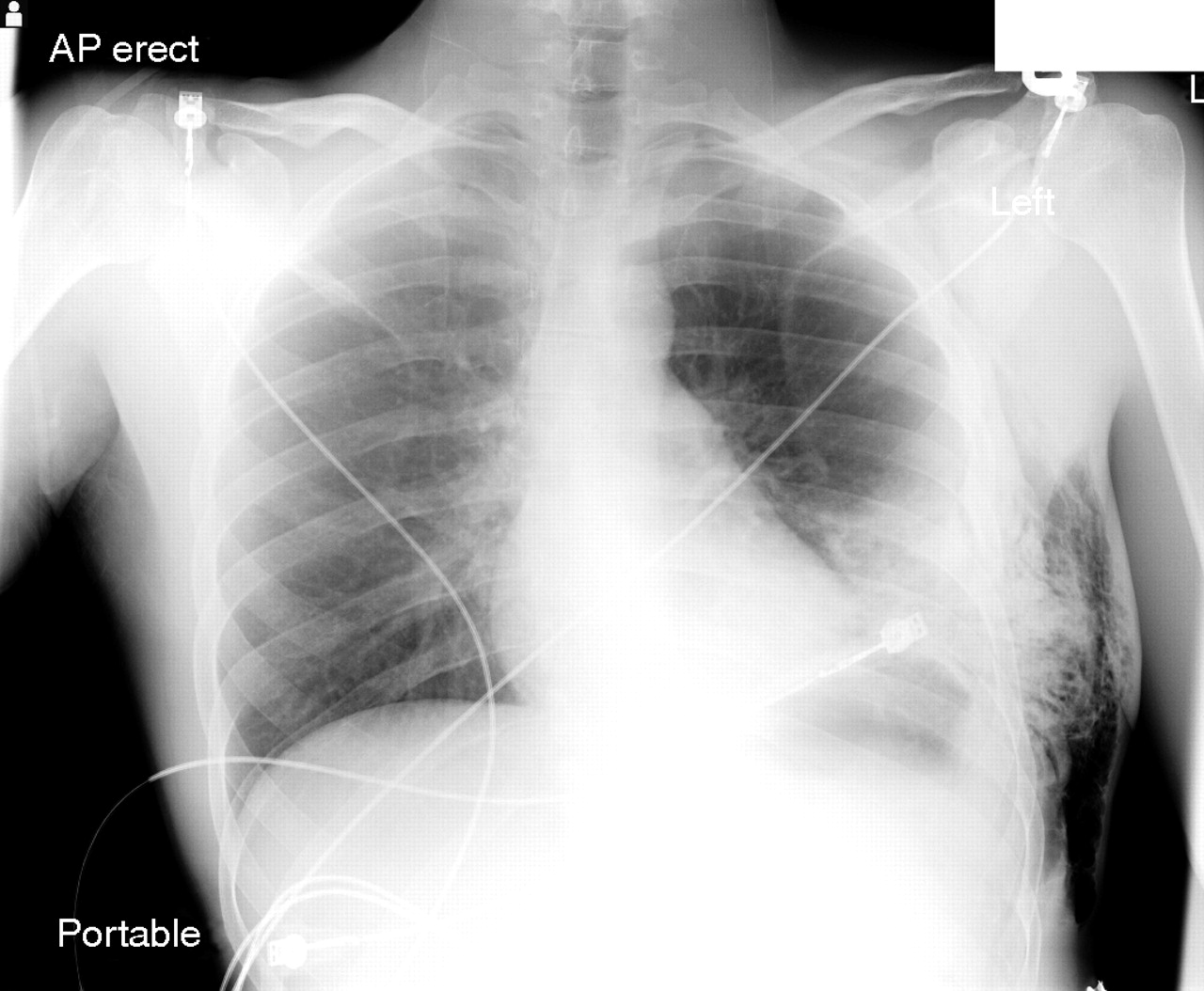{kind=link}
Chest injury secondary attenuated energy projectile.
Footnotes
-
Competing interests: None declared.
Linked Articles
- Primary Survey