

Article Figures & Data
Figures
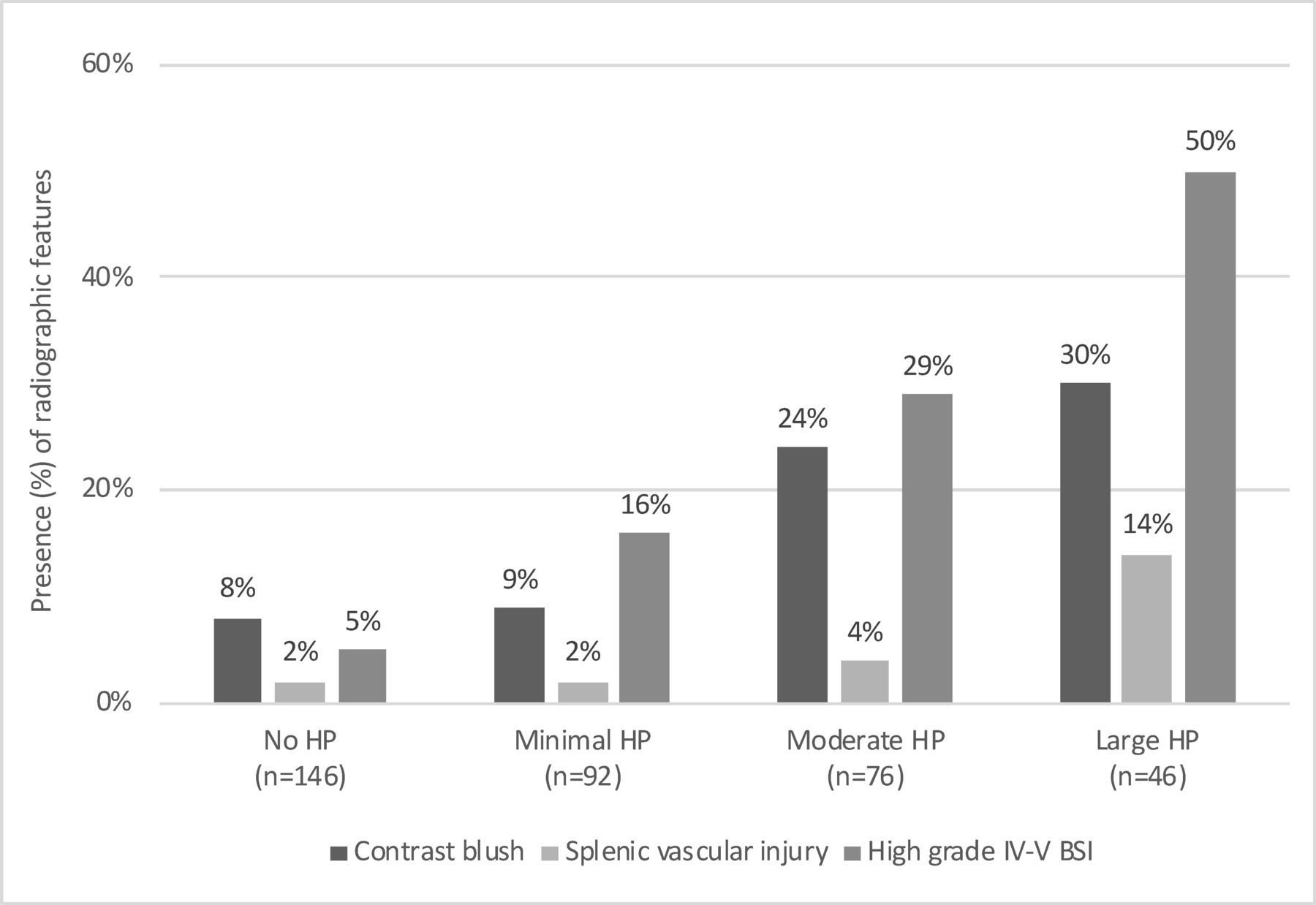
- Figure 1
Presence of radiographic features by quantity of HP. BSI, blunt splenic injury; HP, hemoperitoneum.
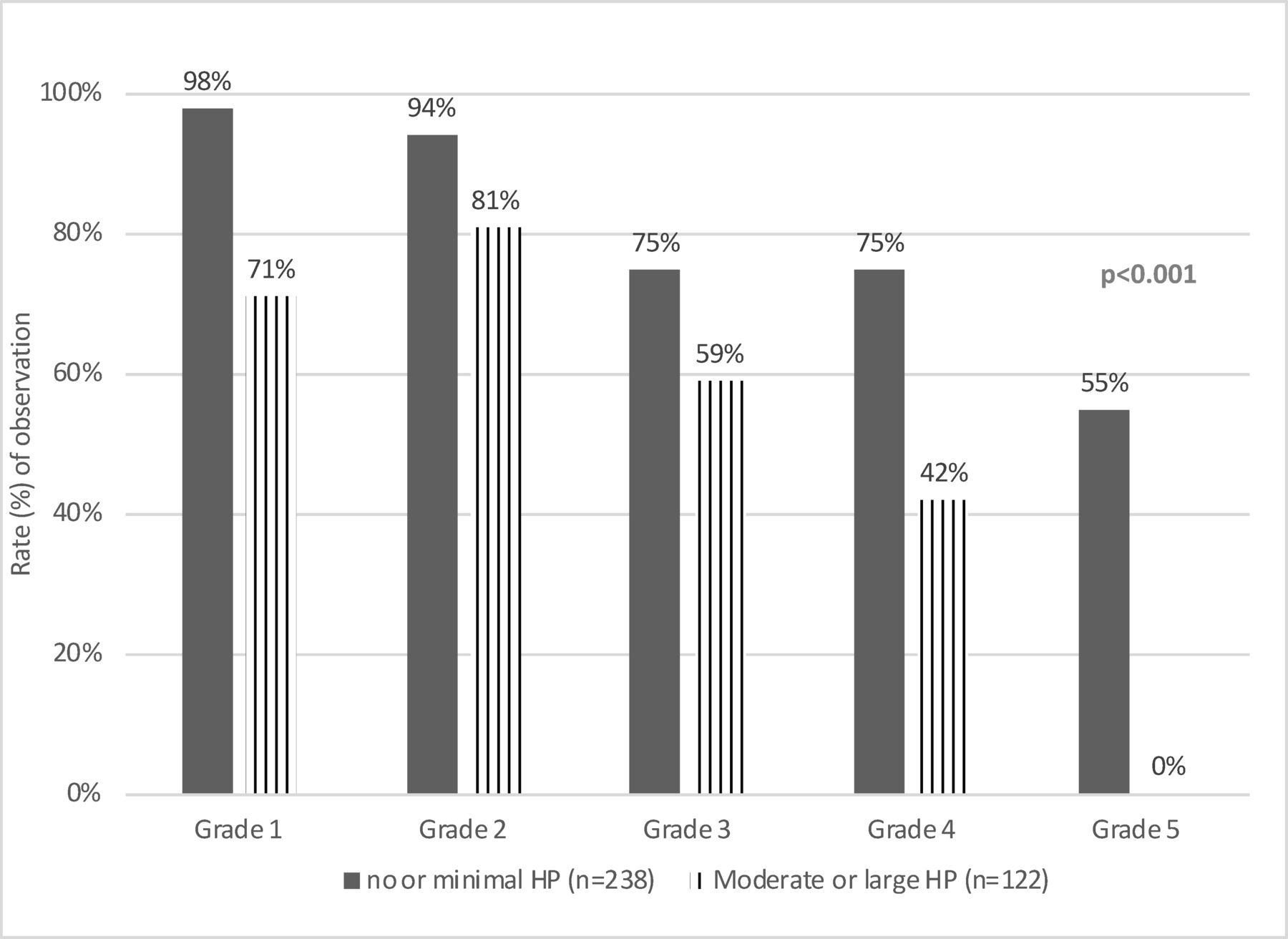
- Figure 2
Rate (%) of observation by quantity of HP and AAST grade. AAST, American Association for the Surgery of Trauma; HP, hemoperitoneum.


Tables
- Table 1
Demographics and clinical characteristics by quantity of HP
Covariate No HP
(n=146)Minimal HP (n=92) Moderate HP (n=76) Large HP
(n=46)P value General characteristics Age, years* 38 (25–55) 36 (25–54) 35.5 (25–55) 30.5 (24–52) 0.51 Age≥65 years 11.0% (16) 6.5% (6) 13.2% (10) 13.0% (6) 0.48 Female sex 37.7% (55) 25.0% (23) 27.6% (21) 37.0% (17) 0.15 Cause of injury 0.24 Vehicular cause 78.1% (114) 78.3% (72) 69.7% (53) 65.2% (30) Fall cause 14.4% (21) 13.0% (12) 13.2% (10) 21.7% (10) Other cause 7.5% (11) 8.7% (8) 17.1% (13) 13.0% (6) ISS* 17 (10–24) 21 (14–29) 17 (10–26) 17 (14–27) 0.04 ED GCS 3–8 13.0% (19) 18.5% (17) 11.8% (9) 6.5% (3) 0.25 ED RR<12 or >20 25.4% (33) 22.7% (20) 27.4% (20) 25.6% (11) 0.92 ED HR>120 10.4% (15) 12.4% (11) 9.2% (7) 10.9% (5) 0.93 Blood type O 30.8% (45) 34.8% (32) 50.0% (38) 39.1% (18) 0.04 First Hb<10ˆ 9.6% (14) 5.4% (5) 10.5% (8) 21.7% (10) 0.03 Radiographic characteristics High AAST grade (IV/V) 5.48% (8) 16.30% (15) 28.95% (22) 50.00 (23) <0.001 Non-surgical abdominal finding 4.1% (6) 6.5% (6) 9.2% (7) 6.5% (3) 0.51 Blush (any) 8.4% (12) 9.1% (8) 24.3% (18) 29.6% (13) <0.001 Splenic vascular injury 2.1% (3) 2.4% (2) 4.2% (3) 13.6% (6) 0.01 Definitive management <0.001 Observation 89.0% (130) 82.6% (76) 56.6% (43) 50% (23) SAE 8.9% (13) 17.4% (16) 42.1% (32) 47.8% (22) fNOM 2.1% (3) 0% 1.3% (1) 2.2% (1) Outcomes Mortality 1.4% (2) 4.4% (4) 5.3% (4) 2.2% (1) 0.35 ICU admission 79.5% (116) 87.0% (80) 92.1% (70) 87.0% (40) 0.07 # blood products* 5 (2–12) 5 (2–8) 3 (2–5) 4 (2–7) 0.56 Hospital LOS* 6 (3–12) 7 (4–14) 6 (4–11) 6 (3–8) 0.33 ICU LOS* 2 (1–5) 3 (2–6) 3 (2–5) 3 (2–4) 0.10 Bold values denote significance <0.05.
*Results presented as median (IQR).
AAST, American Association for the Surgery of Trauma; fNOM, failing nonoperative management; GCS, Glasgow Coma Score; HP, hemoperitoneum; HR, heart rate; ICU, intensive care unit; ISS, injury severity score; SAE, splenic artery embolization.
- Table 2
Demographics and clinical characteristics by definitive management
Covariate Observation (n=272) Intervention* (n=88) P value General characteristics Age, years† 34 (25–53) 42.5 (26–57) 0.03 Age≥65 years 9.2% (25) 14.8% (13) 0.14 Female sex 33.1% (90) 29.6% (26) 0.54 Cause of injury 0.64 Vehicular cause 72.3% (202) 76.1% (67) Fall cause 14.3% (39) 15.9% (14) Other cause 11.4% (31) 8.0% (7) ISS† 17 (10–24) 22 (16–29) <0.001 ED GCS 3–8 13.6% (37) 12.5% (11) 0.79 ED RR<12 or>20 22.3% (56) 33.7% (28) 0.04 ED HR>120 10.1% (27) 12.6% (11) 0.50 Blood type O 33.5% (91) 47.7% (42) 0.02 First Hb<10ˆ 10.3% (28) 10.2% (9) 0.99 Radiographic characteristics High AAST grade (IV/V) 10.29% (28) 45.45% (40) <0.001 Non-surgical abdominal finding 5.2% (14) 9.1% (8) 0.18 Blush 10.3% (27) 27.9% (24) <0.001 HP 52.2% (142) 81.8% (72) <0.001 Splenic vascular injury 1.2% (3) 13.3% (11) <0.001 Outcomes Mortality 2.94 (8) 3.41 (3) 0.82 ICU admission 80.5% (219) 98.9% (87) <0.001 # blood products† 3.5 (2–10) 3 (2–6) 0.45 Hospital LOS† 5 (3–10) 8.5 (5–14) <0.001 ICU LOS† 2 (1–5) 4 (2–8) <0.001 Bold values denote <0.05.
*Intervention: SAE (n=83) or failed NOM (n=5).
†Median (IQR).
AAST, American Association for the Surgery of Trauma; GCS, Glasgow Coma Score; HP, hemoperitoneum; ICU, intensive care unit; ISS, injury severity score; NOM, nonoperative management; SAE, splenic artery embolization.
- Table 3
Logistic regression modeling the need for SAE or failing nonoperative management, vs. successful observation
Covariate OR
(95% CI)P value No HP 1.0 (Ref) Ref Small HP 1.21 (0.46 to 2.76) 0.80 Moderate HP 3.51 (1.49 to 8.26) 0.004 Large HP 2.89 (1.03 to 8.06) 0.03 Age (10-unit increase) 1.25 (1.06 to 1.49) 0.01 Male sex vs. females 1.55 (0.76 to 3.17) 0.23 ISS (10-unit increase) 1.39 (0.96 to 2.00) 0.08 Blood type O vs. other 1.60 (0.83 to 3.07) 0.16 Abnormal RR vs. RR 12–20 1.82 (0.90 to 3.71) 0.10 Blush vs. not 1.39 (0.62 to 3.14) 0.43 Splenic vascular injury vs. not 5.88 (1.12 to 30.99) 0.04 Initial hemoglobin <10 0.52 (0.16 to 1.75) 0.29 BSI grade (continuous) 2.41 (1.68 to 3.47) <0.001 Variables marginally associated in the univariate analysis (p<0.15) were included in the final multivariate logistic regression model. Model fit: AUROC: 0.87; r2=0.47. Bold values denote p<0.05.
AUROC, area under the receiver operating characteristic curve; BSI, blunt splenic injury; HP, hemoperitoneum; ISS, injury severity score; RR, respiratory rate; SAE, splenic artery embolization.
- Table 4
Logistic regression modeling the need for SAE or failing nonoperative management, vs. successful observation: subset of patients with low grade I–III injury and absence of blush and splenic vascular injury (n=258)
Covariate OR
(95% CI)P value No HP 1.0 (Ref) Ref Small HP 0.68 (0.22 to 2.06) 0.49 Moderate HP 5.55 (2.07 to 14.82) <0.001 Large HP 4.88 (1.23 to 19.40) 0.03 Age (10-unit increase) 1.40 (1.12 to 1.74) 0.003 Male sex vs. females 2.77 (1.03 to 7.40) 0.04 ISS (10-unit increase) 1.60 (1.04 to 2.46) 0.03 Blood type O vs. other 1.93 (0.85 to 4.36) 0.12 Abnormal RR vs. RR 12–20 1.28 (0.53 to 3.10) 0.59 Initial hemoglobin <10 0.47 (0.11 to 2.08) 0.32 Variables marginally associated in the univariate analysis (p<0.15) were included in the final multivariate logistic regression model. Model fit: AUROC: 0.80; r2=0.28. Bold values denote p<0.05.
AUROC, area under the receiver operating characteristic curve; HP, hemoperitoneum; ISS, injury severity score; SAE, splenic artery embolization.




{kind=link}
{kind=link}