

Article Figures & Data
Figures
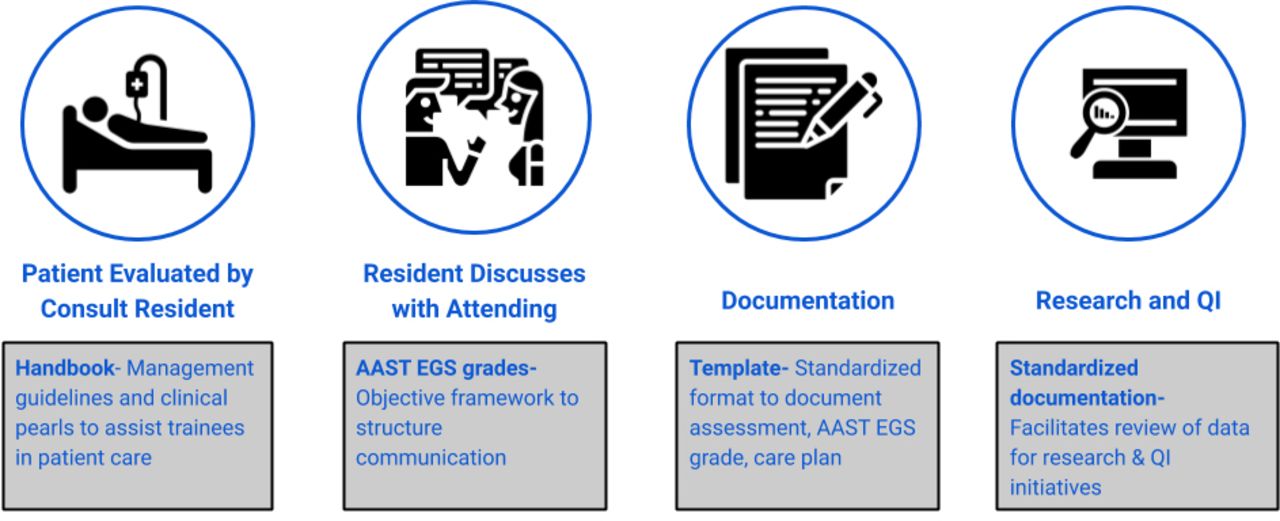
- Figure 1
Schematic of the current acute care surgery clinical workflow. Gray boxes introduce hypothesized improvements as a result of proposed interventions derived from integration of the AAST EGS grading system. AAST, American Association for the Surgery of Trauma; EGS, emergency general surgery; QI, quality improvement.
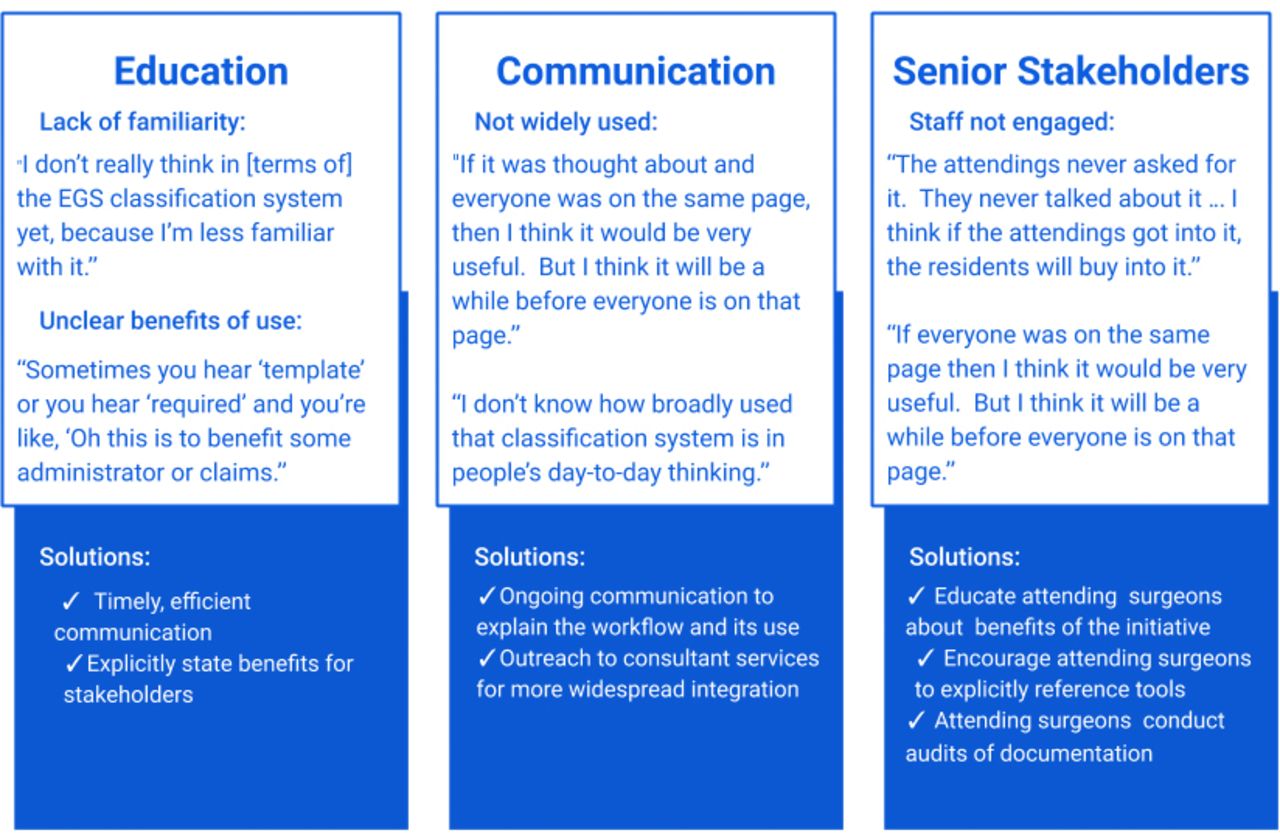
- Figure 2
Barriers to implementation of the AAST EGS grades-integrated workflow identified through qualitative interviews. Obstacles are divided by theme with brief summaries of each perceived obstacle. Quotations illustrate participants’ sentiments toward these issues. Blue boxes outline potential solutions to overcome the aforementioned barriers. AAST, American Association for the Surgery of Trauma; EGS, emergency general surgery.
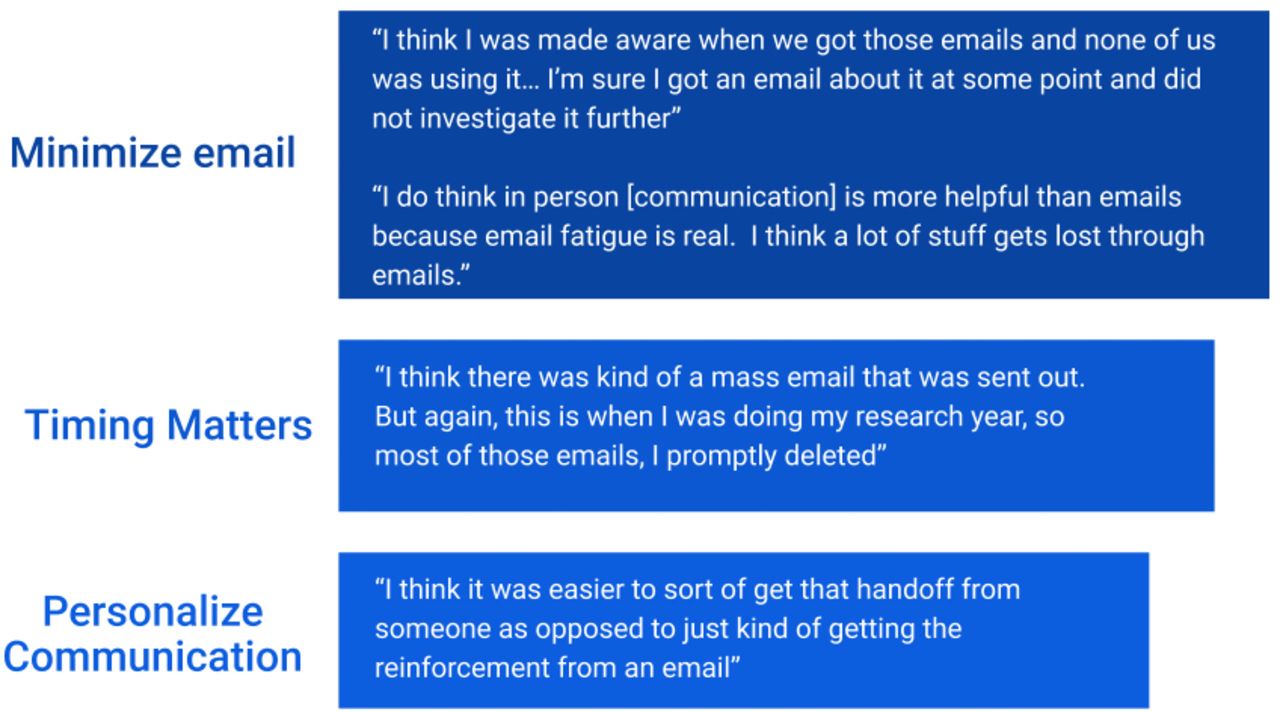
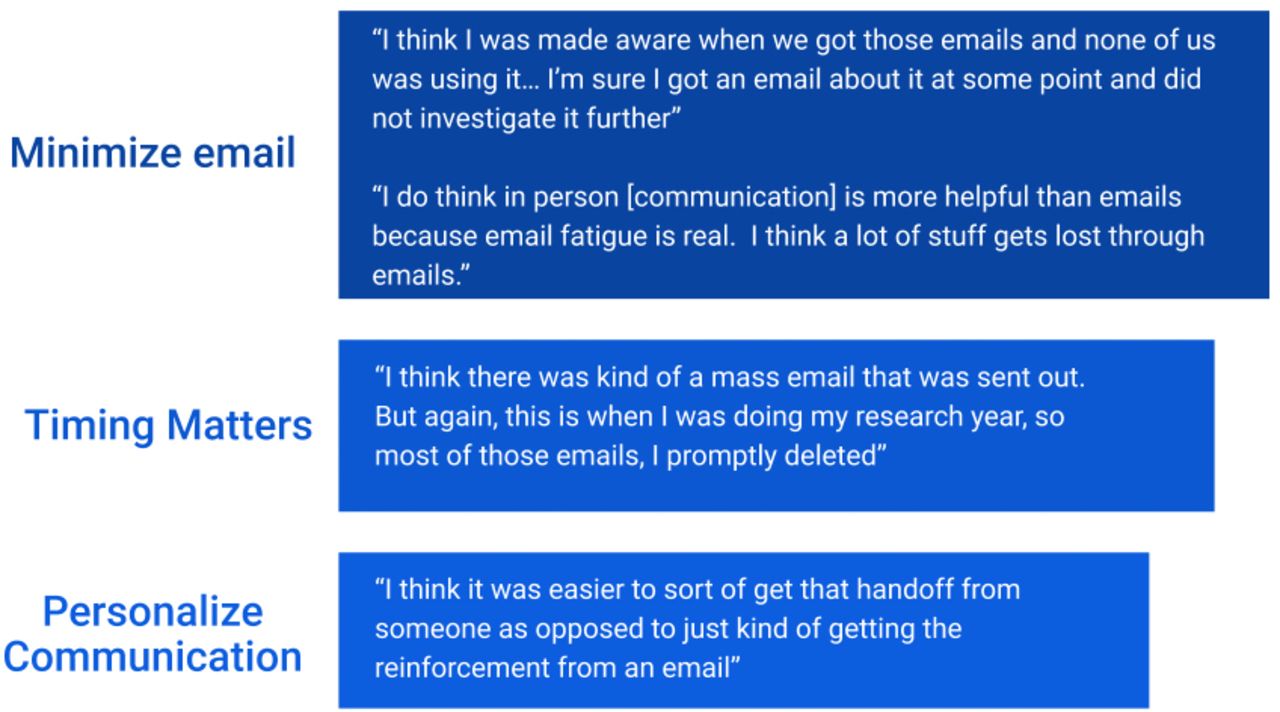
- Figure 3
Best practices to maximize educational endeavors to promote familiarity with an AAST EGS grades-based workflow. Illustrative quotations from interviewees are provided for each. AAST, American Association for the Surgery of Trauma; EGS, emergency general surgery.
Tables
- Table 1
Point-of-care data extraction of patients presenting with emergency general surgery (EGS) conditions between July 30, 2018 and November 18, 2019 using the H&P documentation template
EGS condition Patient encounters (n) Acute appendicitis 370 Peptic ulcer disease 27 Bowel ischemia 13 Small bowel obstruction 403 Colitis 234 Acute diverticulitis 274 Breast infections 329 Acute cholecystitis 384 Acute pancreatitis 172 Soft tissue infections 2 Hernias 28 Perirectal abscesses 55 H&P, history and physical.
- Table 2
Respondents' quotes illustrating the potential of the EGS uniform anatomic severity grading system-based workflow to provide novel opportunities for standardization in care, clinical research, and overall improved patient care
Theme Quotation Standardization ‘The standardization of consult notes is really appealing. Having information that you should always include for common consults, and be able to compare across consults. I think that would be very useful.’ ‘I think that any time appropriate Standardization occurs, then that decreases the potential for human error.’ ‘If this synoptic note and scoring system is validated, it would be really important to have and to use for institutional transfer. You get these calls from community hospitals and you don't have an idea of how acute the patient is. You try to ask enough questions, but then the patients show up here [in a different condition than expected]. I think this being implemented beyond Stanford in general surgery could be really helpful.’ Facilitate clinical research ‘I think it will simplify categorization of patients for research rather than having to sift through dozens of charts later on.’ ‘I would say probably trying to get better data on some of the questions regarding decision making in general surgery. In non-operative management, there are a lot of challenging situations that we make decisions on based on our best judgment and/or discussion with other physicians, but there is little good data to go off. The numbers are small or non-existent. So I think that would be the most useful part.’ ‘Yes, in terms of the guiding data, it is important to know. Because a lot of the patients are probably managed non-operatively and are being missed as important.’ ‘I think you would get lots of good data about the consults we're seeing, how acute they are, how much we're operating, and what we're doing. I think it is a good way to collect data and organize it in an area that would be otherwise hard to follow.’ ‘Where I see value in it is in research. I think it’s similar to organ injury grading for trauma, where at the time of initial evaluation and management, I would say it isn’t particularly useful. I think it is more useful in the backend when it comes to research and classification for studies.’ Improve care ‘I think this is happening in different areas of medicine. Cancer is one example where staging is applied formally. I think it allows you to provide better quality care and to interpret other institutions' information.’ ‘This helps us understand our outcomes. I think that’s motivating for everyone, because everyone wants to help take better of patients and be able to have metrics to know that we’re doing that.’ ‘I think for the first time it will help to really not only classify the types of patients that come to an emergency general surgery service, but it also helps in terms of understanding trends in their care and how we can provide more efficient service to the patients.’ EGS, emergency general surgery.
- Table 3
Respondents’ opinions regarding the use of management guidelines
Benefits of management guidelines Reservations around management guidelines ‘It was really helpful to be able to match the clinical picture I was seeing up to something that was in the consult handbook and then feel comfortable that I making the right management decision for the patient.’ ‘There’s a reason why many physicians don’t adhere to [protocols], because they don’t believe that they apply to the patient population that they're taking care of.’ ‘The consult handbook was especially nice because it was concise, focused on the things we see most often, and I could feel comfortable knowing that I had appropriately assessed the patient and placed them into one of the buckets and that my management decision was going to be in the realm of it was reasonable to treat the patient. It was nice to have that reassurance.’ ‘I think it is possible [to protocolize treatment], but I think it’s never that clean. We just need to find out what emergency cases fit into which category… I think in some ways it’s comparable to injury grading and how we use that, but we may find out it’s not. We don’t really have any data.’ ‘The consult handbook was great, especially starting out, to really guide what to do in these situations and give you the resource quickly make a diagnosis and know “these are the things I need to think about.” It’s not just take them to the OR. It’s also remember to start antibiotics, start fluids, and these ancillary details might get lost in all the focus of “this patient has got to go to the OR”.’ ‘I think for straightforward things it’s probably a good idea. Like for proven appendicitis or cholecystitis. But, I think for other kinds of emergency general surgery consults, like perforated viscus, you have no idea if its upper GI or lower GI. Perhaps the pathway for those scenarios is probably not the best thing and might lead people to the wrong route.’ ‘I think with any grading or classification system, it provides a rubric and a starting point with suggested management based on disease severity, but you’re not obligated to do that regardless of what your team ends up doing, it provides a baseline, agreed upon management and I think that is only going to be helpful.’ ‘There are definitely times when the patient falls in between 2 different classes, but you’re supposed to use your clinical judgment to be able to determine what their treatment is. That’s the fault of any classification system. Sometimes there is gray. It’s not always black and white.’ ‘Having a classification system with a clear outline on what management steps we take, what tests to order, what studies to be done. I think that lets us make sure we don't miss any important workups or plans.’ ‘I mean the residents may use that, but I don’t think the faculty member is going to pull up a handbook. They’re just not, it doesn’t fit the workflow.’ ‘I think that with the diagnostic information being brought in through the EGS classification system, it’s going to really stratify branch points and management based on classification systems of these typical emergency general surgery problems.’ ‘Sometimes I feel like there is almost a discrepancy between what my assessment and plan is as compared to the a few words that are in the classification itself. I think sometimes there’s a little bit of a disconnect there. Sometimes I would think to myself “is it ok to say other or select this criteria even if its not 100% applicable to the patient in one way but it is in another?”’ ‘It makes it much more black and white in terms of how to communicate about the patient. I also provides a little bit of a checklist in the middles of the night when you're tired to make sure you don't forget anything.’ ‘I think you’re going to run into the same problem where you have now a second layer of “how do I interpret these guidelines?” I’m not sure how much it will be helpful, because the decision making process in always complicated no matter what. Patients are not that straightforward and they may not fit into certain guidelines. If the guidelines are written very carefully with definite hard points where there is certain criteria where for like 95% certainty this next step should happen, then I think it would be useful.’
Supplementary data
Supplementary data




{kind=link}
{kind=link}
{kind=link}