

Abstract
A 69-year-old obese man was involved in a high-speed head-on motor vehicle collision. He was tachycardic and normotensive on arrival. He subsequently developed hemodynamic instability requiring blood transfusion. On examination he had bilateral pneumothoraces, an anterior-posterior compression (APC) pelvic fracture, an open wound at the left groin, and gross hematuria after Foley catheter placement.
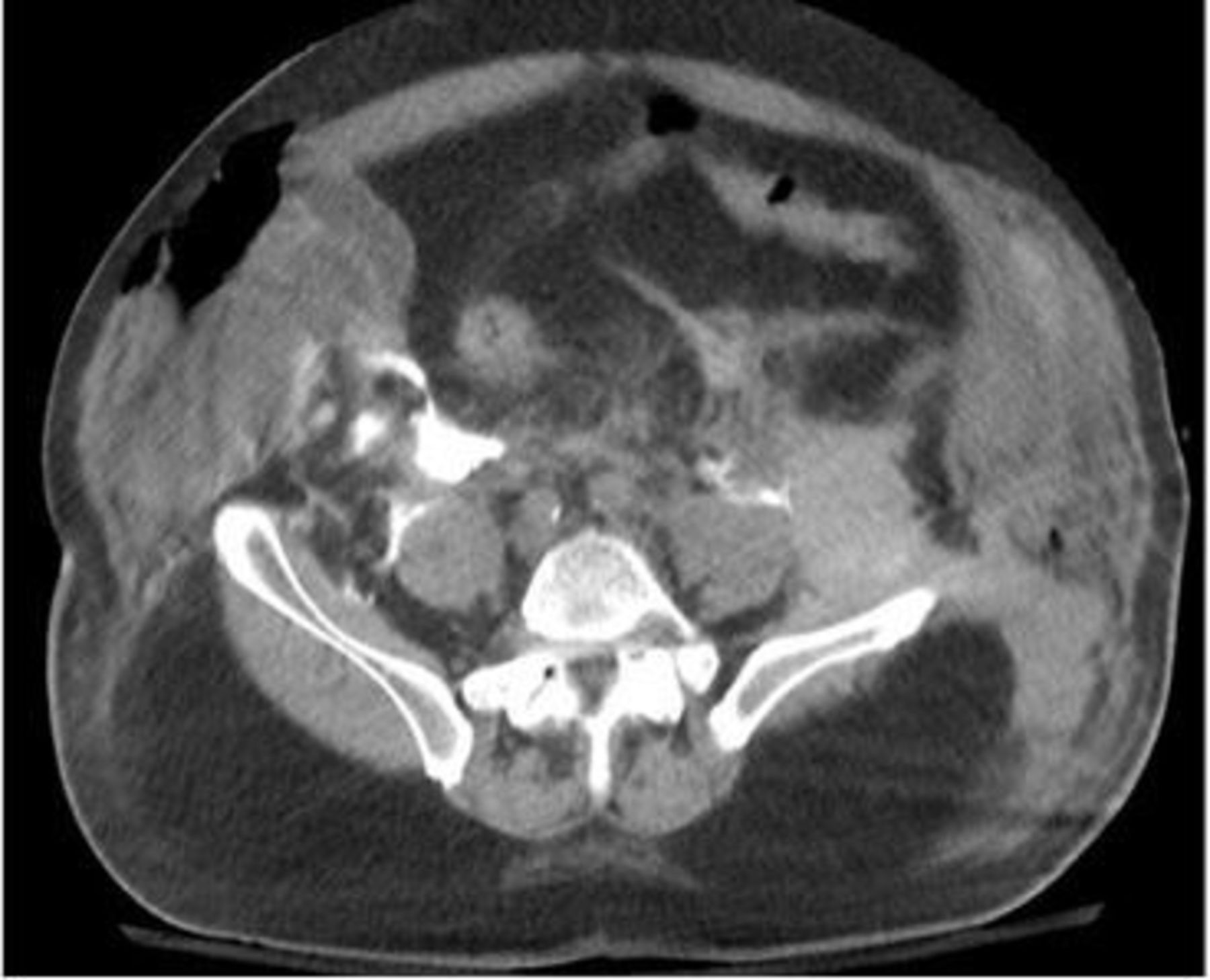
CT imaging revealed hemoperitoneum, right hepatic lobe grade II lacerations, splenic laceration, mesenteric root injury with extravasated contrast, intraperitoneal and extraperitoneal bladder rupture, bilateral ureteral injuries at the level of the pelvic inlet (see figure 1), APC pelvic fracture, bilateral rib fractures, pneumothoraces, and pulmonary contusions.

CT of the abdomen and pelvis with cystogram. Delayed images demonstrating accumulation of contrast in the retroperitoneum arising from the right and left ureter at the level of the pelvic brim. Extraluminal contrast from the intraperitoneal bladder injury is also identified.
He underwent emergent exploratory laparotomy. Exploration confirmed the injuries noted on the CT scan. Hepatorrhaphy with abdominal and preperitoneal pelvic packing was performed. A large anterior bladder wall injury was visualized. Neither ureteral orifice was seen. The right ureter was completely transected at the level of the pelvic brim. The left ureter was decompressed and the full extent of its injury was not determined; however, the bladder injury left concern for a distal avulsion. The patient continued to be in shock.
Reconstruct the urinary bladder and reimplant bilateral ureters.
Ligate the ureter and prepare for pelvic embolization and nephrostomy tubes.
Continue to explore looking for the full extent of the left ureter.
Externalize the ureters to the abdominal wall with the open abdomen.
What we did and why
Correct answer: B
The urologic injuries required complex repair, and the patient was in shock. Damage control techniques were employed. The peritoneal and preperitoneal spaces were packed and the right ureter was ligated. He was taken to interventional radiology for angioembolization of his retroperitoneum and pelvis, as well as percutaneous nephrostomy tubes.
Although lumbar vessels (L4–L5) and a branch of the left internal iliac artery were embolized, the patient’s physiology continued to worsen. Percutaneous nephrostomy tubes were not performed. His abdomen was re-explored, repacked and hemostasis verified. He was taken to the surgical intensive care unit for further resuscitation. Continuous renal replacement therapy began for hyperkalemia due to prerenal and renal causes.
On hospital day 2, he underwent re-exploratory laparotomy and complex urologic reconstruction with the assistance of urology. A distal left ureteral transection was confirmed in addition to the known right ureter transection. Left ureteral reimplantation was performed over a ‘double-J’ ureteral stent. All bladder injuries (anterior wall and dome) were repaired. A ‘single-J’ urinary diversion stent was placed retrograde in the distal right ureter and externalized through the abdominal wall.
He continued to have profound hypotension postoperatively with increasing vasopressor requirements. On hospital day 3 he developed severe acute respiratory distress syndrome. Over the following days he developed acute liver failure, required electrical cardioversion for rapid atrial fibrillation, and developed sepsis from Gram-negative rod bacteremia. He remained in shock, refractory to resuscitative efforts with worsening hypoxia despite maximal ventilator support. Due to multisystem organ failure a compassionate wean was performed on hospital day 5.
Complications of ureteral injuries include retroperitoneal abscess, urinomas, strictures, fistulae, renal failure, sepsis, and death. The operative management of blunt ureteral transection in the hemodynamically unstable patient is focused on damage control with urinary diversion. Initial ureteral injury management includes externalization by stenting, or ligation of the proximal ureter with placement of a nephrostomy tube. A ureteral injury may also drain spontaneously for a short period of time, but is best avoided if alternatives exist. Urine creates a significant inflammatory reaction and increases the risk of delayed sepsis. Broad-spectrum intravenous antibiotics should be started to prevent colonization and clinical infection.
It may have been prudent to place ‘single-J’ ureteral stents in both ureters and externalize them for drainage at the index operation or at the second operation. This would have controlled urinary extravasation. The urinary bladder would have been defunctionalized and could have been reconstructed later. This may have decreased the second-look operative time and helped improve his physiology during this critical phase of attempted rescue.
Patients with blunt traumatic ureteral injury are often critically ill due to multiple associated injuries (such as this patient with an Injury Severity Score of 75). They require prompt identification of their injuries and a staged reconstructive approach to decrease morbidity and mortality. Extensive definitive urinary system repairs are best performed when the patient has resolved their shock state. Until then, damage control techniques should be used.
Footnotes
Funding Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}