

Article Figures & Data
Figures
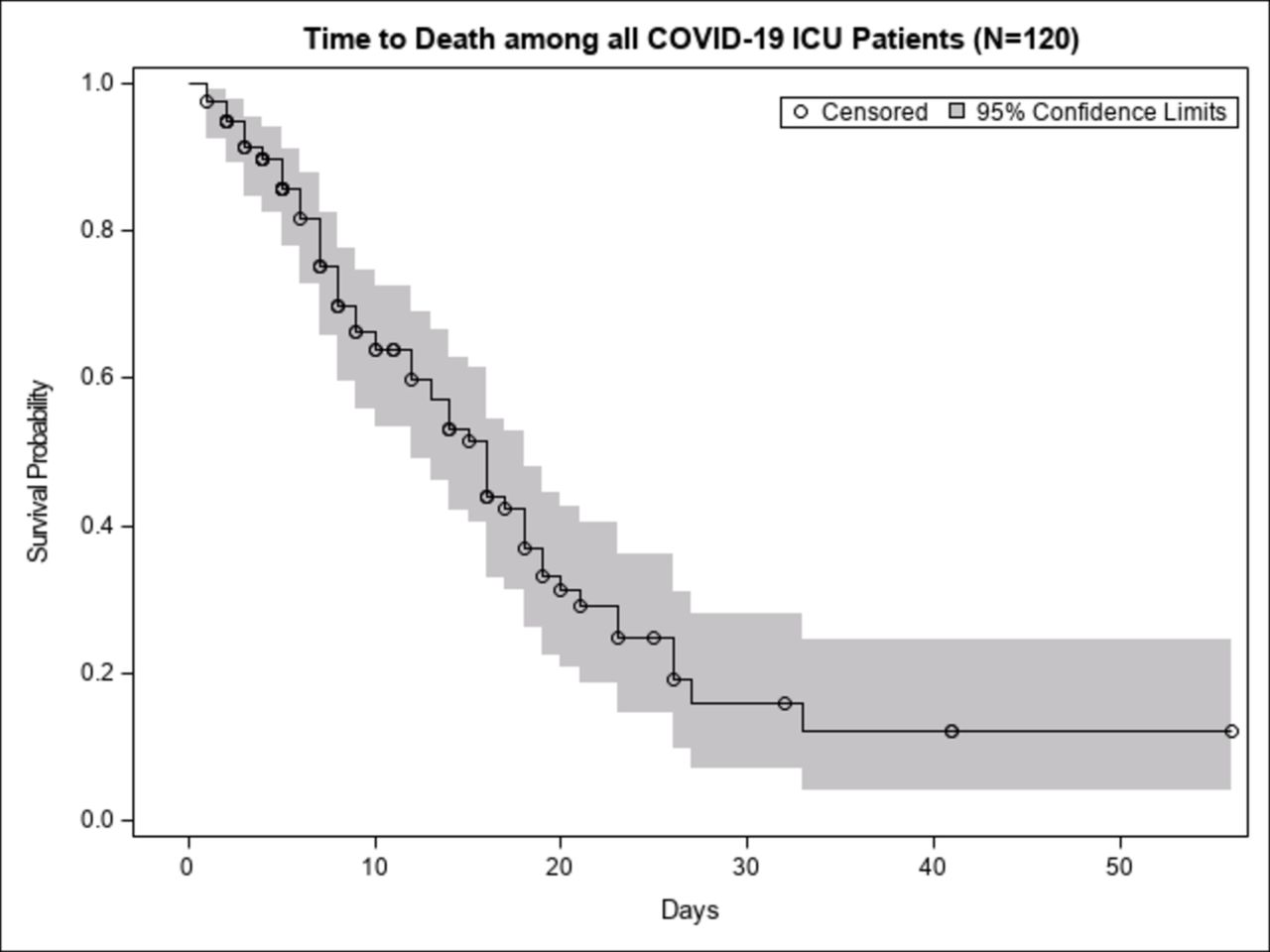
- Figure 1
Survival of critically ill patients with COVID-19 in an acute care surgery intensive care unit (ICU).
Tables
- Table 1
Baseline Characteristics of Critically Ill Patients with COVID-19 (n=120)
n % Demographics Age (years), median (IQR) 120 64 (17.5) Sex, male 80 66.7 Race/ethnicity* Caucasian 55 45.8 Black 16 13.3 Hispanic 38 31.7 Asian 11 9.2 Comorbidities† None 19 15.8 Chronic respiratory disease Chronic obstructive pulmonary disease/asthma 12 10.0 Obstructive sleep apnea 7 5.8 Diabetes 50 41.7 Obesity Body mass index >30 kg/m2 61 50.8 Body mass index >35 kg/m2 26 21.7 Cardiovascular disease Hypertension 75 62.5 Heart failure 13 10.8 Coronary artery disease 21 17.5 Myocardial infarction 7 5.8 Chronic kidney disease 11 9.2 End-stage renal disease requiring dialysis 2 1.7 Cirrhosis 2 1.7 Immunocompromised 7 5.8 Rheumatologic disease 7 5.8 Cognitive disability 16 13.3 Signs and symptoms Cough 82 68.3 Shortness of breath 75 62.5 Fever 71 59.2 Lethargy 54 45.0 Diarrhea 13 10.8 Previous presentation 49 40.8 Primary care provider 27 22.5 Emergency department 12 10.0 Hospital admission 10 8.3 Exposure to COVID-19 Travel to high-risk area 4 3.3 Family member with COVID-19 15 12.5 Healthcare-related exposure 4 3.3 Group home 9 7.5 Nursing home 16 13.3 Unknown 72 60 *Race and ethnicity data were collected by self-report.
†Comorbidities listed were medical diagnoses included in the medical history defined by ICD-10 coding.
- Table 2
Vital Signs, Laboratory Results, and Treatments of Critically Ill Patients with COVID-19 (n=120)
n Median IQR Admission vital signs Temperature degrees Fahrenheit 120 100.10 3.35 Heart rate (beats per minute) 120 99.00 25.50 Systolic blood pressure (mm Hg) 119 130.00 32.00 Mean arterial pressure 119 92.00 23.00 Initial O2 saturation 118 90.00 13.00 Admission laboratory results White cell count (×109/L) 120 7.67 27.72 Absolute lymphocyte count (×109/L) 120 6.00 7.95 Sodium (mmol/L) 120 135.00 5.50 Creatinine (mg/dL) 120 1.00 0.72 Total Bilirubin, mg/dL 119 0.50 0.34 Alkaline phosphatase (IU/L) 120 78.00 39.00 Aspartate aminotransferase (U/L) 120 50.00 39.00 Lactate (mmol/L) 114 1.80 1.40 Basic natriuretic peptide (pg/mL) 44 546.30 1622.00 Troponin (ng/mL) 108 0.02 0.02 Troponin above 0.02, n (%) 4 3.3% Procalcitonin (ng/mL) 106 0.36 0.78 Hemoglobin (g/dL) 120 13.20 2.70 Platelets (x109/L) 119 211.00 129.00 International normalized ratio (s) 102 1.00 0.10 Prothrombin time (s) 99 10.90 1.50 HbA1c (%) 52 6.80 1.85 Admission studies Bilateral infiltrates on chest X-ray, n (%) 104 86.7% Chest CT scan obtained, n (%) 26 21.7% False-negative COVID-19 tests, n (%) 6 5.0% Highest value during hospitalization Lactate dehydrogenase (U/L) 113 550.00 292.00 Ferritin (ng/mL) 112 1140.00 1433.00 Triglycerides (mg/dL) 83 186.00 184.00 D-dimer (mg/L) 104 4.30 12.12 Fibrinogen (mg/dL) 73 633.00 272.00 Temperature peak degrees Fahrenheit 117 103.10 1.60 Lowest value during hospitalization pH nadir 115 7.21 0.27 Lowest P/F ratio 115 73.00 63.00 Hydroxychloroquine 94 78.3% Azithromycin 83 69.2% Remdesivir 17 14.2% Tocilizumab 45 37.5% Convalescent plasma 10 8.3% Pharmacological paralysis 35 29.2% Proning 29 24.2% Vasopressor requirement 89 74.2% P/F, arterial oxygen partial pressure to fractional inspired oxygen.
- Table 3
Acute Respiratory Distress Syndrome (ARDS) and COVID-19-Related Complications in Critically Ill Patients with COVID-19 (n=120)
n % ARDS* 113 94.2 Mild ARDS 4 3.3 Moderate ARDS 28 23.3 Severe ARDS 81 67.5 Infectious complications† Bacterial pneumonia 40 33.3 Urinary tract infection 22 18.3 Bacteremia 22 18.3 Influenza 0 0.0 Clostridium difficile 3 2.5 High-grade fever (>103 degrees Fahrenheit) 59 49.2 Acute kidney injury‡ 76 63.3 Renal replacement therapy 28 23.3 Acute hepatic injury§ 8 6.7 Venous thromboembolism¶ Deep vein thrombosis 3 2.5 Pulmonary embolism 3 2.5 Cardiac complications** Arrhythmia 31 25.8 Myocardial infarction 4 3.3 Cardiomyopathy 8 6.7 Pneumothorax†† 8 6.7 Neurological complications‡‡ Seizures 3 2.5 Cerebrovascular accident 2 1.7 Intracranial hemorrhage 2 1.7 Gastrointestinal bleed 6 5.0 Tracheostomy 7 5.8 Percutaneous gastrostomy tube 5 4.2 *ARDS was defined by Berlin definition with bilateral infiltrates on chest radiograph along with a P/F ratio <100 for severe ARDS, between 100 and 200 for moderate ARDS, and between 200 and 300 for mild ARDS.
†Infectious complications were defined as positive lower respiratory tract, urine, or blood cultures respective to pneumonia, urinary tract infection, and bacteremia. Positive respiratory viral panel with respect to influenza. Positive PCR for C. difficile.
‡Acute kidney injury was defined as an increase in serum creatinine by ≥0.3 mg/dL within 48 h or an increase of at least 1.5 times baseline within 7 days.
§Acute hepatic injury was defined as an elevation of aspartate aminotransferase or alanine aminotransferase greater than 15 times the upper limit of normal.
¶Venous thromboembolism was defined by new image-proven deep vein thrombosis in femoral or popliteal veins on venous duplex ultrasonography or pulmonary embolism on CT angiography.
**Cardiac complications were defined as a new arrhythmia requiring intervention, clinically relevant non-ST-elevation myocardial infarctions and ST-elevation myocardial infarctions, and transthoracic echocardiography revealed depressed contractility and function with respect to cardiomyopathy.
††Pneumothorax was defined by chest radiograph.
‡‡Neurological complications defined new-onset seizures by electroencephalogram, and new ischemic lesions and intracranial hemorrhage by CT or MRI.
- Table 4
Outcomes for Critically Ill Patients with COVID-19
Outcome of
ICU patients with COVID-19Age group (years) All patients (n=120) 20–40
(n=5)41–60
(n=41)61–80
(n=64)81–90
(n=10)Length of ICU stay (days) (IQR) 9 8 8.5 8 8.5 (9) Length of hospital stay (days) 15 15 14.5 15 14.5 (13) Still hospitalized (discharged from ICU) 1 2 4 1 8 (6.7%) Discharged from hospital 1 20 27 0 48 (40%) Discharged on oxygen 1 3 6 – 10 30-day readmission 0 1 1 – 2 Required invasive
mechanical ventilation (IMV)4 34 54 8 100 (83.3%) IMV at admission 1 12 22 1 36 (36%) Hospital days prior to IMV, median* 2.0 3.0 3.0 2.0 3.0 IMV days, median 8.5 7.0 10.5 5.0 9.0 Died after IMV 3 (75%) 19 (55.9%) 32 (59.3%) 8 (100%) 62 (62%) Mortality 3 (60%) 19 (46.3%) 33 (51.5%) 9 (90%) 64 (53.3%) Died with DNI (never received IMV) 0 0 1 1 2 Died with DNR 2 13 29 8 52 Died with comfort care 1 9 17 6 33 Died with severe ARDS, n=81 3 17 17 7 54 Died with moderate ARDS, n=28 1 5 2 8 *Median number of hospital days prior to ventilation, calculated among those that did not require ventilation at admission.
ICU, intensive care unit; DNI, do not intubate; DNR, do not resuscitate; ARDS, acute respiratory distress syndrome.




{kind=link}