

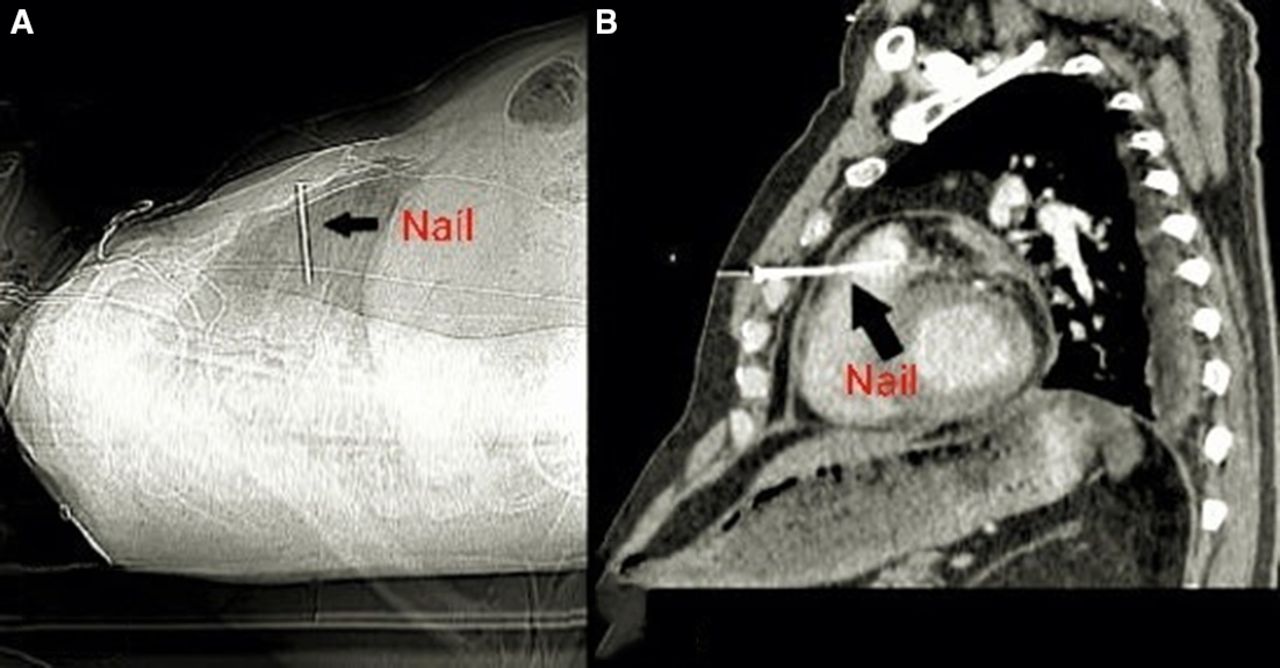
A patient in his 50s shot himself with a nail gun presented to our center for further management after initial resuscitation in district general hospital. An echocardiogram report demonstrated mild pericardial effusion; he was hemodynamically stable at the time of admission. An urgent chest CT scan was performed which showed a nail in the left hemithorax between the fourth and fifth intercostal space anteriorly medial to the nipple, and the tip of the nail appeared to be in the pericardial space, next to the right ventricular outflow tract and left basal anterior wall without sign of perforation (figure 1 A,B). The pericardium was mildly thickened at the site of the nail entry and a small pericardial effusion of approximately 8 mm. There was no sign of vascular or cardiac structure perforation neither contrast leak. In addition, there was a small left pleural effusion which suggested a possible hemorrhagic component; a small amount of air was noted in the left pectoral muscle with no fractured bone.

A and B, The CT scan showed a nail in the left hemithorax between the fourth and fifth intercostal space medial to the nipple, and the tip of the nail appeared to be in the pericardial space.
What would you do?
1. Explore the chest with median sternotomy, thoracotomy or video-assisted thoracoscopic surgery (VATS) to remove the nail.
What we did and why
The radiology department was consulted, and a CT scan confirmed no involvement of the vascular, cardiac, or major lung structures except pericardium which influenced our surgical decision to consider other approaches apart from sternotomy or thoracotomy. Moreover, hemodynamic stability encouraged less invasive procedure.
The patient was transferred to the theatre for nail extraction. Under general anesthesia and intubation, the patient’s hemodynamics were monitored using invasive arterial blood pressure and Central Venous Pressure (CVP) continuous measurement. A transesophageal echocardiogram (TEE) was performed which confirmed previous findings. The cardiopulmonary bypass machine was primed and kept as standby ready to be used in case of hemodynamic instability.
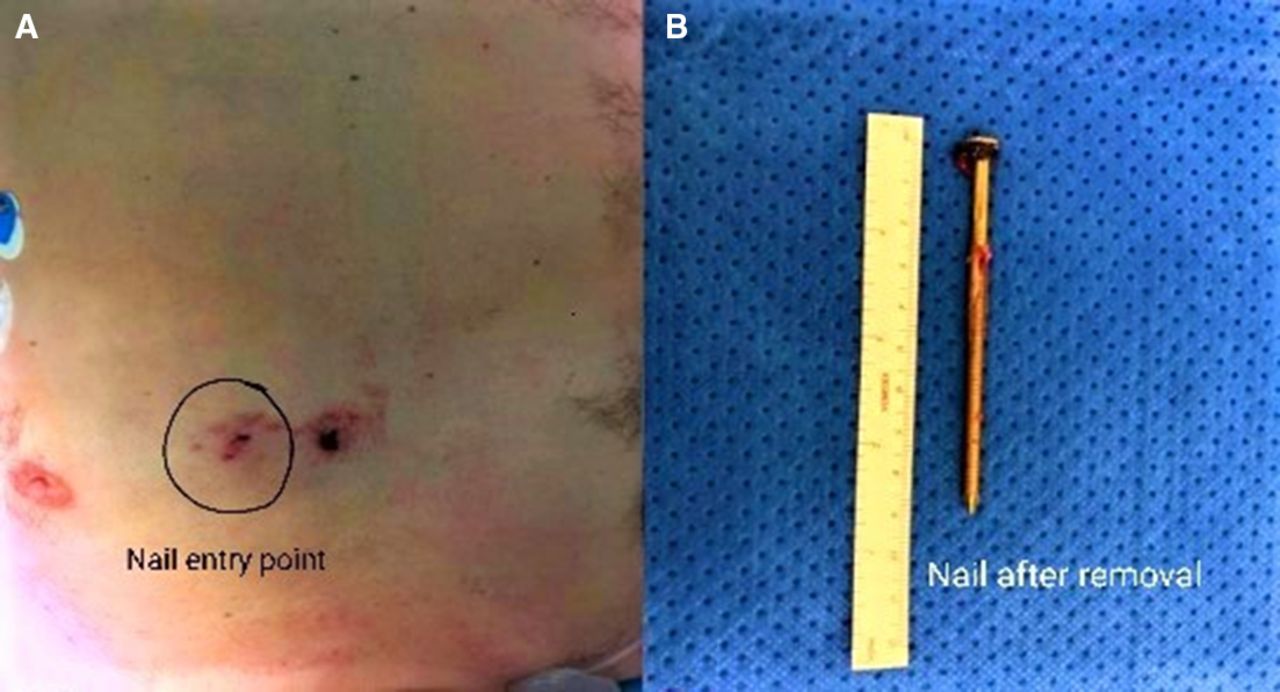
In theatre, the patient was in a supine position and prepared for median sternotomy. The nail entry point on the skin was explored through a 3 cm incision (figure 2). The nail was pulled out under TEE guidance(figure 3). It provided real-time visualization of cardiac structures and monitored for an increase in the pericardial collection which remained unchanged after removal of the nail. Afterwards, the patient was transferred to Intensive Therapy Unit (ITU) and was monitored. He was sedated until the next morning when another TEE was performed to check the change in pericardial effusion. After ensuring no change in the pericardial collection, sedation was stopped, and the patient was extubated.

(A)Nail entry point and (B) nail after removal.
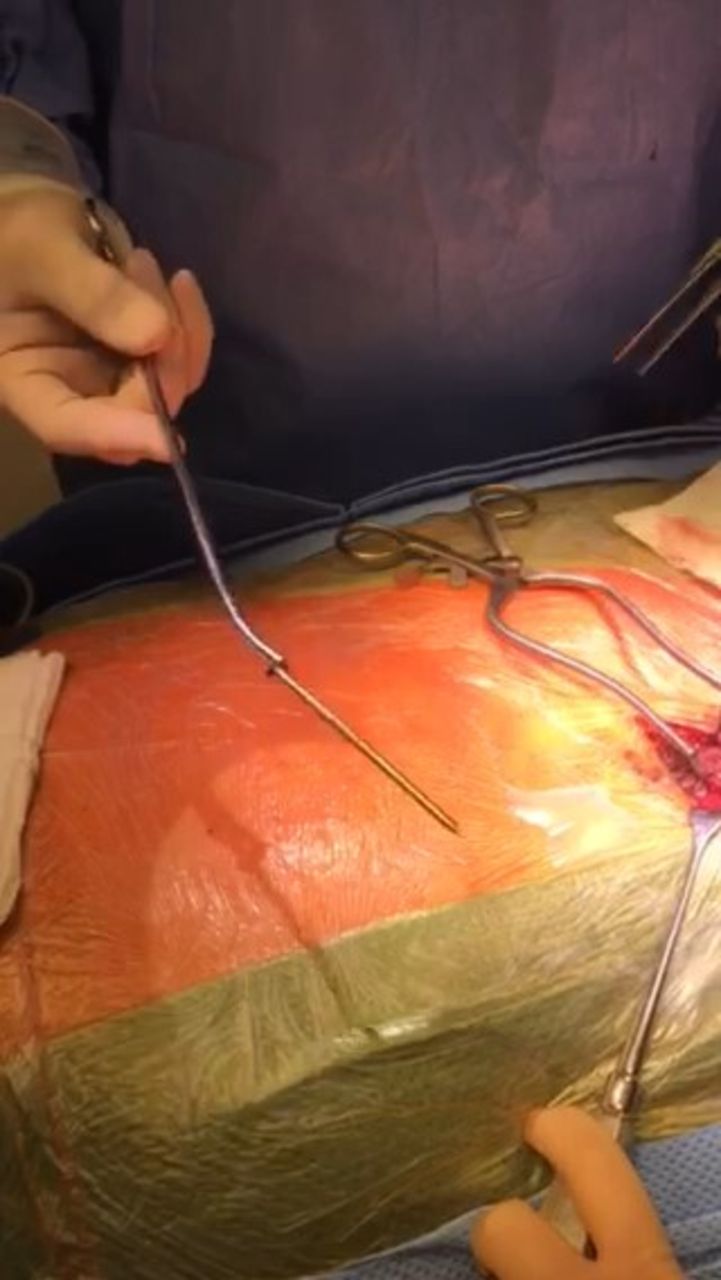
Nail removal through a small incision in the injury site.
The patient stayed stable for the next 48 hours. On the 5th postoperative day, the patient was discharged with painkiller and antibiotics treatment as he was hemodynamically stable, and the wound site looks normal.
Discussion
This is an unusual case of nail extraction from the left anterior chest and pericardium without opening the chest. It was explored by merely a small incision at the injury site. Median sternotomy is an excellent incision in cases with cardiac trauma and provides better access to great vessels for cannulation for cardiopulmonary bypass and heart. On the other hand, clamshell incision provides better exposure to both thoracic cavities. However, morbidity and wound dehiscence associated with both the median sternotomy and clamshell incision. Moreover, it makes future cardiac surgery more challenging.
Thoracotomy also is a recommended incision for cardiothoracic trauma, as it provides good exposure to the heart. It does not need sternal saw; thus, it can be used in case of emergency. VATS is another option in this case as it is less invasive than sternotomy and thoracotomy, but it provides limited access to anterior surface of the heart especially if right ventricular repair was needed. Thus, the choice was to start with small incision and proceed to sternotomy if needed.
With thorough reviewing of the available imaging modalities, continuous monitoring and having a backup plan in case of hemodynamic instability, we managed to avoid chest opening in this case. Evaluation by CT scan and continuous monitoring by TEE was the key for effective management. CT scan is an excellent imaging modality that provides position of the nail and excluded major cardiac or vascular injury or the presence of pericardial effusion. TEE provided us with continuous imaging before and during nail extraction to exclude pericardial effusion and tamponade during the procedure.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable, as the patient provided written informed consent and this case report does not include any identifiable information.
Footnotes
Contributors RB was directly involved in the planning, writing, conception of design, analysis, review, revision and proofreading of the publication, and agreed to follow the rules of publication in the journal. MO was directly involved in the planning, writing, conception of design, analysis, review, revision and proofreading of the publication, and agreed to follow the rules of publication in the journal. MR was directly involved in the writing, conception of design, analysis, review, revision and proofreading of the publication, and agreed to follow the rules of publication in the journal. LD'E was involved in the review, revision and proofreading of the publication, and agreed to follow the rules of publication in the journal. KS was involved in the review, revision and proofreading of the publication, and agreed to follow the rules of publication in the journal. CN was involved in the review, revision and proofreading of the publication, and agreed to follow the rules of publication in the journal.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. However, received fund for APC from Royal Papwortyh Charity.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}