

Case description
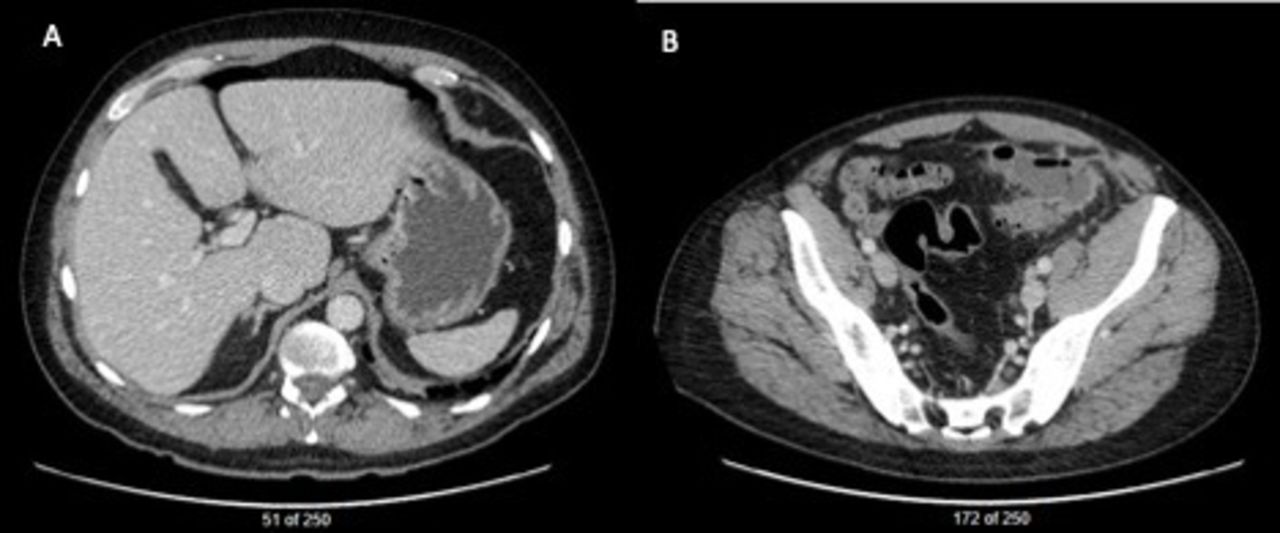
A middle-aged man, with a medical history of rheumatoid arthritis (treated with methotrexate) and gastroesophageal reflux disease presented to a community hospital with a 1-day history of abdominal pain. A CT scan abdomen/pelvis revealed acute diverticulitis with extensive sigmoid colon inflammation but no abscess. The patient was clinically well and non-peritonitic so intravenous antibiotics were initiated. He was later discharged home with oral antibiotics and a referral for outpatient colonoscopy. Approximately 6 weeks later, colonoscopy identified severe diverticulosis and internal hemorrhoids, but no evidence of malignancy. After colonoscopy, the patient returned to the community hospital with severe left lower quadrant (LLQ) abdominal pain. Laboratory investigations revealed a C-reactive Protein of 132 and neutrophilia leukocytosis White Blood Cell Count 11.1). A CT scan abdomen/pelvis demonstrated an abscess collection (7×3.5×6 cm) in the LLQ, persistent sigmoid colon thickening, and multiple scattered pockets of free intraperitoneal air (figure 1). The CT report diagnosed perforation of the colon either from diverticulitis or recent colonoscopy. Fluid resuscitation and broad-spectrum intravenous antibiotics were initiated. The patient was transferred to a tertiary care hospital for surgical management. On arrival, the patient was reassessed by the surgical team and found to be peritonitic but hemodynamically stable. Consent for a laparotomy, possible bowel resection, and possible stoma was obtained.

CT scan on representation to emergency department after colonoscopy showing (A) pockets of free air in upper abdomen, (B) fluid and gas-filled collection in left lower quadrant.
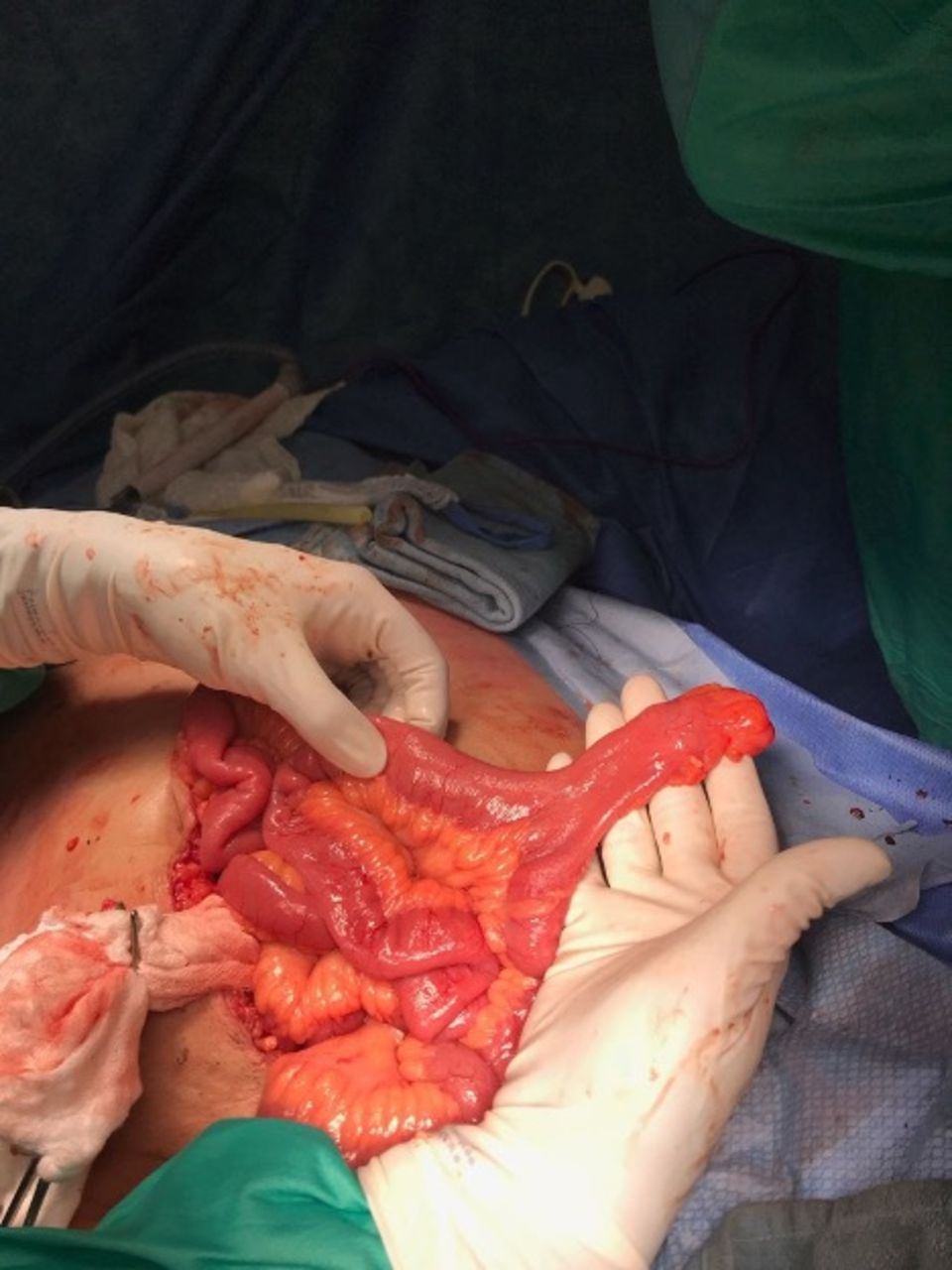
Intraoperative findings confirmed severe diverticulitis. A large abscess was encountered in the LLQ with purulent contamination, consistent with modified Hinchey III classification. The sigmoid colon was thickened and inflamed. Incidentally, a Meckel’s diverticulum (MD) was noted at approximately 35–40 cm from the ileocecal valve. The diverticulum was approximately 10 cm long with a 2 cm base, and there was no gross or palpable abnormality appreciated (figure 2). The patient remained hemodynamically stable throughout the case.

Incidental Meckel’s diverticulum found near the location of planned diverting ileostomy site.
What would you do?
Sigmoid resection with end colostomy (Hartmann’s procedure)
Sigmoid resection, primary anastomosis
Sigmoid resection, primary anastomosis; with diverticulectomy and distal loop ileostomy
Sigmoid resection, primary anastomosis; with small bowel resection at site of Meckel’s diverticulum with anastomosis and distal loop ileostomy
Sigmoid resection, primary anastomosis; with small bowel resection at site of Meckel’s diverticulum with double barrel ileostomy
Sigmoid resection, primary anastomosis; and Meckel’s diverticulectomy as loop ileostomy site
What we did and why?
Correct answer: F
Given purulent contamination in bilateral lower quadrants, immunocompromised patient, and significant fecal loading, it was not safe to perform a sigmoid resection and primary anastomosis alone. Therefore, sigmoid resection with primary anastomosis and proximal fecal diversion was considered most appropriate for this patient. The optimal site of a diverting loop ileostomy was near the incidental MD, presenting a challenge in this case. A Hartmann’s procedure would have been the most conservative approach, however, primary anastomosis with proximal diversion was favored given higher rates of stoma reversal without additional morbidity. Additionally, a Hartmann’s procedure would not address the MD. Other options (3, 4, and 5) were excluded given the risk of additional staple lines, anastomosis, and potential for small bowel devascularization with mesenteric division.
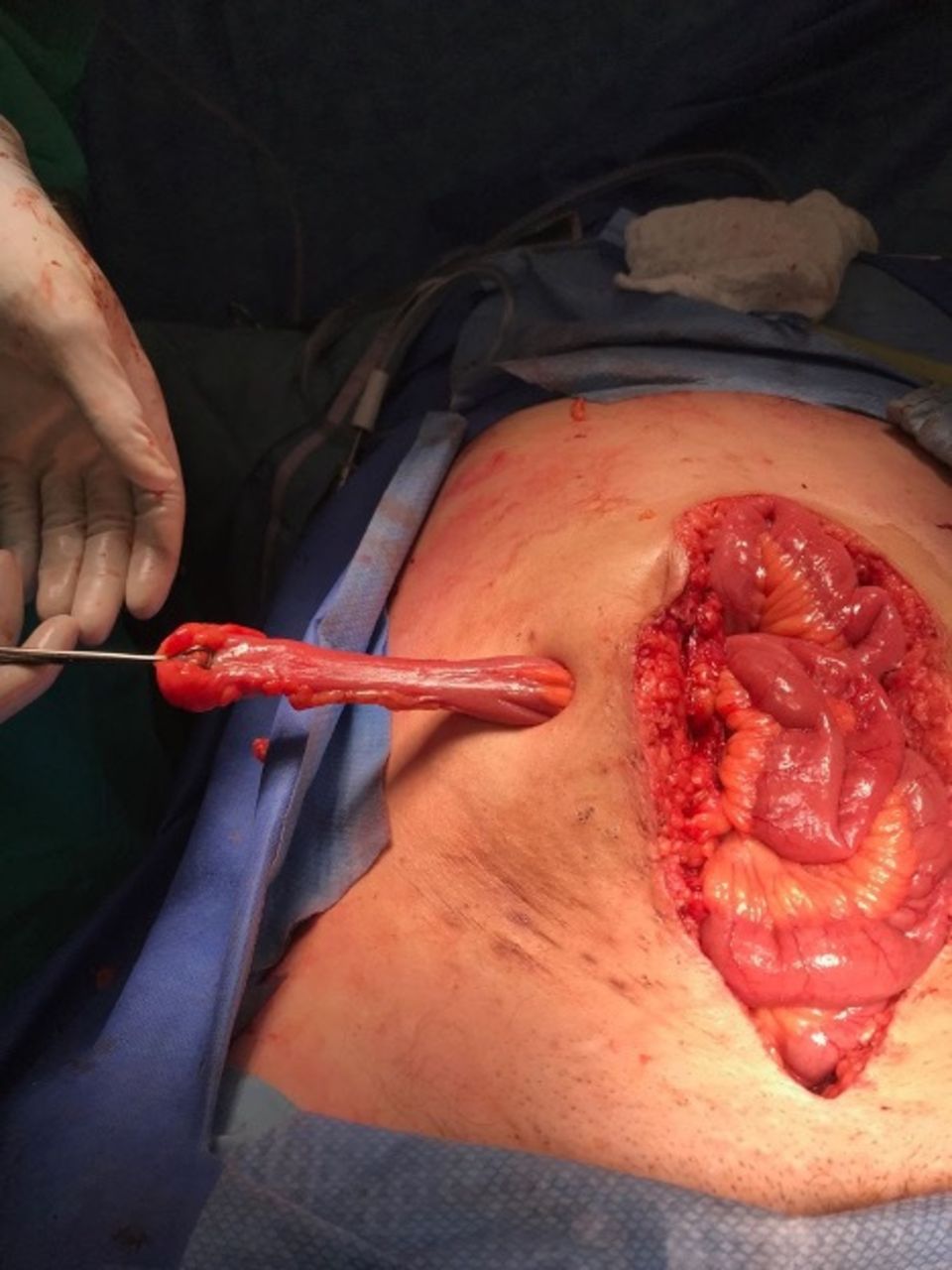
Resection is recommended when an incidental, asymptomatic MD has any of these factors: patients less than 50 years old, narrow base, length greater than 2 cm, palpable abnormality, or a fibrous band connecting the diverticulum to the umbilicus. The presence of any of these factors significantly increases the risk of future complications, with multiple factors increasing cumulative risk. In this case, the MD was narrow based and long (>2 cm). Moreover, the patient was immunocompromised, and future complications related to the MD could be problematic. Finally, the patient’s age supported resection for risk mitigation. Thus, the decision was made to perform a diverticulectomy, and use this site as the loop ileostomy. A standard ostomy orifice was created in the right lower quadrant. The MD was extirpated through the orifice (figure 3), then transected at its base using a linear tissue stapler. The staple line was removed to create a loop ileostomy.

Meckel’s diverticulum brought out through right lower quadrant ileostomy site prior to diverticulectomy.
The postoperative course was significant for a small surgical site infection managed by wound opening and conventional packing. By postoperative day 2, there was return of bowel function via loop ileostomy. The patient was discharged home on postoperative day 7. Final pathology revealed chronic and active diverticulitis without malignancy in the colon specimen, and benign small bowel mucosa with focal adhesions but without heterotopic mucosa in the MD. At 12 weeks postoperatively, loop ileostomy reversal was performed after confirming integrity and patency of anastomosis by cross-sectional imaging with rectal contrast. This procedure was uncomplicated and tolerated well. Final pathology was benign. Most recent follow-up revealed no complications.
Operative management of perforated diverticulitis continues to evolve and the chosen approach ultimately depends on patient and disease factors encountered during surgery. The Hartmann’s procedure is the most traditional and conservative approach. More recently, sigmoidectomy with primary anastomosis and loop ileostomy has gained favor with similar short-term outcomes, and possibly better long-term outcomes in relation to stoma-free status at 1 year. Our case highlights two challenges for the acute care surgeon. First, managing perforated diverticulitis in the immunocompromised patient; and second, navigating an incidental MD in close proximity to an optimal loop ileostomy location. We describe a novel approach to this dilemma by creating a loop ileostomy at the site of MD. We would recommend this approach to others who encounter similar pathology.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors contributed to the creation of this manuscript including idea development, and writing and editing the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}