

Case presentation
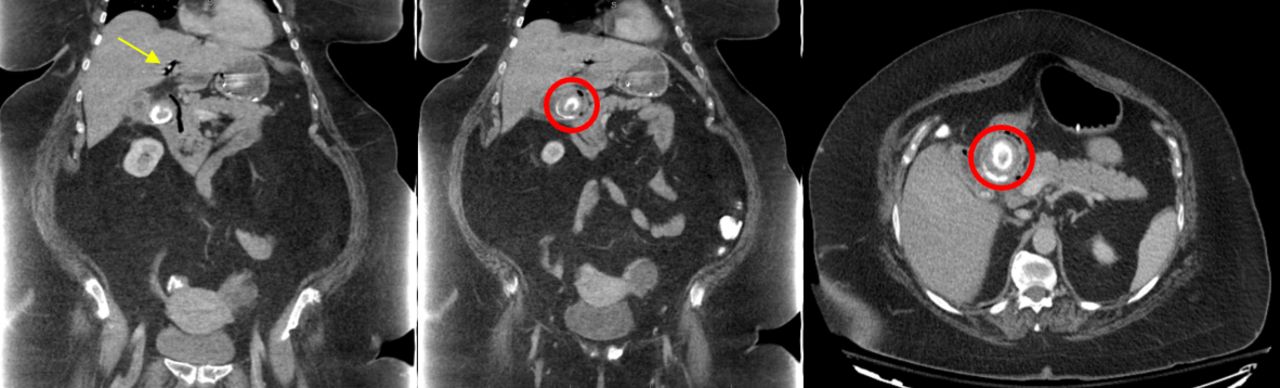
A 62-year-old woman presented to the emergency department complaining of 2 weeks of right upper quadrant and epigastric pain that acutely worsened 5 days prior to admission. This was associated with nausea and vomiting. Her medical history was significant for morbid obesity (body mass index 67 kg/m2), hypothyroidism, hypertension, congestive heart failure and multiple cerebrovascular events on therapeutic rivaroxaban. Her abdomen demonstrated moderate epigastric tenderness without peritoneal signs. Laboratory values were all normal. CT of the abdomen and pelvis with oral and intravenous contrast showed a large gallstone causing partial gastric outlet obstruction and pneumobilia (figure 1).

Multiple cuts of the CT scan showing gastric outlet obstruction caused by a large gallstone in the duodenum (red circle) with associated pneumobilia (yellow arrow).
What would you do?
Endoscopic retrieval of stone.
Endoscopic electrohydraulic and/or mechanical lithotripsy.
Laparotomy with enterolithotomy and cholecystoenteric fistula closure.
Laparotomy with enterolithotomy without cholecystoenteric fistula closure.
What we did and why
A nasogastric tube (NGT) was inserted for gastric decompression, and a myocardial perfusion scan and echocardiogram were obtained, which demonstrated no myocardial ischemia and normal left ventricular function (ejection fraction of 50% to 55%). She then underwent upper endoscopy during which a 5 cm gallstone was identified in the duodenal bulb adherent to the duodenal mucosa, approximately 2 to 3 cm distal to the pylorus. These findings, in tandem with Rigler’s triad of gastric outlet obstruction, a gallstone in the duodenum and pneumobilia confirmed the diagnosis of a cholecystoduodenal fistula (figure 2).
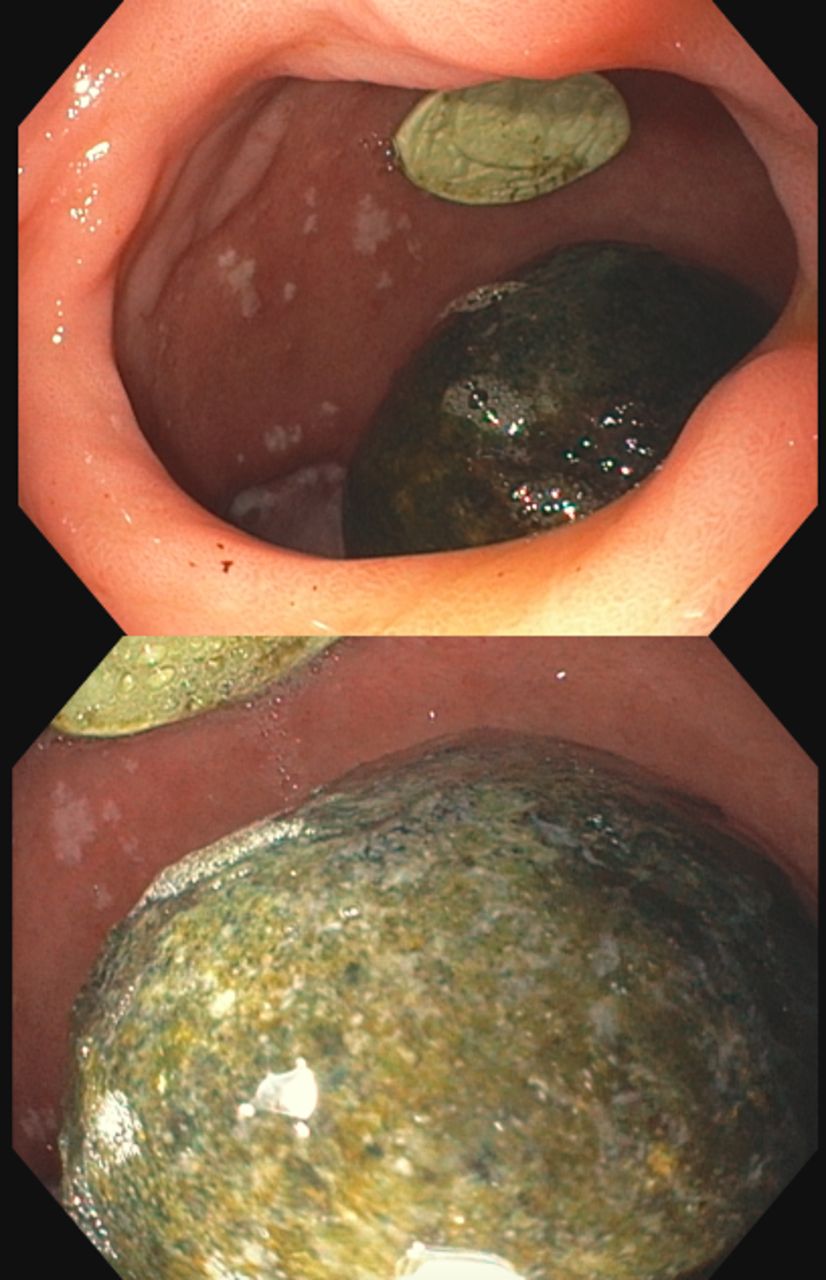
Obstructing gallstone identified in D1 during endoscopy.
Bouveret syndrome is an exceedingly rare etiology for gastric outlet obstruction. The majority of cases occur in patients over 70 years old; thus, they frequently have multiple comorbidities and extensive surgical histories. With the main goal of therapy being gallstone removal, endoscopy remains a useful modality. Existing literature, though scarce, describes the success of endoscopic interventions, such as electrohydraulic lithotripsy or manual extraction, of gallstones up to 3 cm in size. Our patient did have a complex medical history for which a simpler procedure would be preferred. However, the encouraging results of her cardiac function tests, the large size of the stone on CT scan and inability to traverse the obstruction prompted a more invasive therapeutic plan. Fortunately, she was clinically stable on admission, which did allow proper preoperative optimization.
While minimally invasive approaches to foregut and biliary surgery are becoming increasingly predominant, the extent of inflammation appreciated on imaging as well as the significant anatomic distortion caused by the disease process were factors favoring an open approach to safely maximize visualization. After discussing these considerations among all members of the surgical team, the patient subsequently underwent an exploratory laparotomy. The duodenum was found to be densely adherent to inferior edge of the liver. Traction sutures were placed at the superior and inferior margins of the pylorus, and an anterior gastrotomy was created, extending across the pylorus by 2 cm in either direction. The large 5.5 cm stone was extracted carefully to avoid future distal obstructions from fragmentation (figure 3). A nasojejunal tube for early enteral nutrition and NGT for decompression were placed under direct visualization.

Gross images of the 5.5 cm gallstone extracted intraoperatively from the duodenum.
At this point, the question of fistula repair was discussed. Importantly, no additional cholelithiasis within the gallbladder was identified on imaging studies or during intraoperative evaluation. Additionally, the extensive adhesions encountered in the porta hepatis and periduodenal region would have likely made further dissection of the hepatocystic triangle and adjacent fistulous tract exceptionally challenging. To minimize the associated risk of enteral and biliary injury, fistula closure was not pursued. Instead, a pyloroplasty was performed using the Heineke-Mikulicz technique in two layers with 3–0 Vicryl and 3–0 Silk suture. A modified Graham patch was then used to buttress the pyloroplasty. The bowel was then run in its entirety, to rule out distal obstruction. The patient’s postoperative course was uncomplicated. She tolerated a regular diet on postoperative day 5, was discharged on postoperative day 6 and was fully recovered at her 2-week follow-up visit. On recovery from the acute episode, referral to hepatobiliary surgery for cholecystectomy and definitive fistula closure should be discussed with patients diagnosed with Bouveret’s syndrome. This patient, however, wished not to pursue further surgical evaluation or interventions as she was content with her current quality of life.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but was not approved by A human subject was involved, however we did not provide any experimental treatments. The standard of care was provided. Furthermore, all images and patient identifiers were deidentified. Thus IRB approval was not deemed necessary. Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors AACC participated in conceptualization, planning, design, article writing and article editing. NRS participated in design, article writing and article editing. SHC participated in acquisition of data, conceptualization, planning, design and article editing. JPW participated in conceptualization, planning and article editing. All authors provided final approval of article and figures prior to submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.




{kind=link}
{kind=link}
{kind=link}